Welcome to IgMin Research – an Open Access journal uniting Biology, Medicine, and Engineering. We’re dedicated to advancing global knowledge and fostering collaboration across scientific fields.
Welcome to IgMin, a leading platform dedicated to enhancing knowledge dissemination and professional growth across multiple fields of science, technology, and the humanities. We believe in the power of open access, collaboration, and innovation. Our goal is to provide individuals and organizations with the tools they need to succeed in the global knowledge economy.
IgMin Publications Inc., Suite 102, West Hartford, CT - 06110, USA
Background: Zinc deficiency has been identified as a contributing factor to poor appetite, impaired immune function, and various gastrointestinal disturbances in young children.
Objective: To assess the effect of zinc supplementation on vomiting status in anorexic children.
Methods: A randomized, controlled, single-blinded clinical trial. Fifty vomiting anorexic children (3–36 months old) without infection and gastro-intestinal outlet obstructions were selected on admission to the nutrition recovery center: 25 (supplemented, S group) received 10mg/child daily of elemental zinc supplementation as gluconate with iron and vitamins of supplemental dosage, and 25 (non-supplemented, NS group) received a similar one but without zinc for 90 days. All children were also observed during a 90-day post-supplementation period, one child of the S group and four children of the NS group dropped out. On days 7, 10, and 15 the vomiting status was assessed. On days 0 and 30, the levels of energy intake and weight gain were measured. On days 0 and 90, serum zinc levels were also measured.
Results: On days 7, 10, and 15, the healed proportions of the vomiting children were significantly higher (83.3% vs. 0.0%; 87.5% vs. 4.8% and 95.5% vs. 19%) in the S group than that in the NS group (p < 0.001 for each). On day 30, the levels of energy intake (108 ± 20 vs. 82 ± 16 Kcal/kg/day) and weight gain (414 120 vs. 248 ± 102 g/child/mo) were significantly higher in the S group than in the NS group (p < 0.001 for each). Serum zinc levels (µg/dl) were significantly higher (76.8 ± 8.4 vs. 71.2 ± 6.3, p < 0.05) in the S group than in the NS group on day 90.
Conclusion: This study supports the role of zinc in protracted vomiting not due to gastro-intestinal outlet obstructions in anorexic children, while pointing out the need for large studies.
Vomiting is a common symptom with various underlying causes. It is essential to consider organic diseases, especially when vomiting is prolonged or severe [11Ravindranath A. Chronic vomiting in children: Etiology, diagnosis, and management. Indian J Gastroenterol. 2020 Apr;39(2):117-122. doi: 10.1007/s12664-020-01035-w. PMID: 32385612.]. Vomiting can also be indicative of serious gastrointestinal disorders [22Vomiting in Children: Clinical Scenarios. Current Treatment Options in Pediatrics, 2023; 9(1): 1-14. https://doi.org/10.1007/s40746-023-00283-0.]. In children, prolonged vomiting can significantly hinder the intake of energy and nutrients, leading to malnutrition and potentially severe complications [33Malnutrition: Definition, Causes, Symptoms & Treatment. Cleveland Clinic. 2022. Available at: https://my.clevelandclinic.org/health/diseases/22987-malnutrition]. Identifying and addressing the underlying causes of vomiting is crucial in treatment, but in many cases, the cause remains unclear, leading to symptom-based treatment and frequent relapses. Therefore, determining the root cause of vomiting is essential for effective management.
Zinc plays a vital biological role in reducing vomiting through its influence on various molecular and cellular mechanisms. Zinc is a cofactor for numerous enzymes, such as carbonic anhydrase, alkaline phosphatase, and alcohol dehydrogenase [44Namakin K, Sharifzadeh GR, Zardast M, Khoshmohabbat Z, Saboori M. Comparison of the WHO Child Growth Standards with the NCHS for Estimation of Malnutrition in Birjand-Iran. Int J Prev Med. 2014 May;5(5):653-7. PMID: 24932399; PMCID: PMC4050688.], which are critical for maintaining cellular function, metabolism, and acid-base balance. Its involvement in regulating ion channels and stabilizing cellular membranes further enhances its protective role in gastrointestinal health [55Bryant-Waugh R, Markham L, Kreipe RE, Walsh BT. Feeding and eating disorders in childhood. Int J Eat Disord. 2010 Mar;43(2):98-111. doi: 10.1002/eat.20795. PMID: 20063374.]. Zinc also exerts an anti-inflammatory effect by modulating cytokine production and immune response, which may help alleviate irritation and inflammation of the gastrointestinal lining-a potential contributor to vomiting [66Jha VM, Jha SK. Sleep: Disorders and Clinical Implications. In: Sleep: Evolution and Functions. Springer, Singapore. Sleep: Evolution and Functions. 2020;101-118. https://doi.org/10.1007/978-981-15-7175-6_6.]. Additionally, zinc is known to influence neurotransmitter function, particularly serotonin and dopamine, which are involved in the vomiting reflex. By stabilizing these neurotransmitter pathways, zinc may help in reducing nausea and vomiting [77International Zinc Nutrition Consultative Group (IZiNCG); Brown KH, Rivera JA, Bhutta Z, Gibson RS, King JC, Lönnerdal B, Ruel MT, Sandtröm B, Wasantwisut E, Hotz C. International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr Bull. 2004 Mar;25(1 Suppl 2):S99-203. PMID: 18046856.].
During our observation of digestive disorders in anorexic children, we noted that those who experienced vomiting showed rapid improvement in both vomiting and anorexia symptoms following zinc supplementation [88Somji SS, Dhingra P, Dhingra U, Dutta A, Devi P, Kumar J, Deb S, Semwal OP, Sazawal S, Manji K, Kisenge R, Bakari M, Aboud S, Liu E, Sudfeld C, Duggan CP, Ashorn P, Bahl R, Simon JL. Effect of dose reduction of supplemental zinc for childhood diarrhoea: study protocol for a double-masked, randomised controlled trial in India and Tanzania. BMJ Paediatr Open. 2019 Apr 24;3(1):e000460. doi: 10.1136/bmjpo-2019-000460. Erratum in: BMJ Paediatr Open. 2020 Oct 12;4(1):e000460corr1. doi: 10.1136/bmjpo-2019-000460corr1. PMID: 31206083; PMCID: PMC6542451.]. This observation aligns with prior research demonstrating the efficacy of zinc supplementation in reducing vomiting episodes in children with acute diarrhea [99Dewey KG, Brown KH. Update on technical issues concerning complementary feeding of young children in developing countries and implications for intervention programs. Food Nutr Bull. 2003 Mar;24(1):5-28. doi: 10.1177/156482650302400102. Erratum in: Food Nutr Bull. 2003 Jun;24(2):239. PMID: 12664525.]. These findings suggest that zinc's effects may extend beyond diarrhea to other vomiting-associated conditions. Consequently, we conducted this study to investigate the effect of zinc supplementation on prolonged vomiting in anorexic children.
A randomized, controlled, single-blinded clinical trial was conducted at the Rehabilitation Center for Malnourished Children in Ho Chi Minh City, Vietnam. Fifty children aged 3–36 months with a history of vomiting and anorexia lasting over a week were enrolled. Children with acute infections or gastrointestinal obstructions were excluded.
The study targeted children aged 3–36 months with symptoms of vomiting and anorexia lasting at least one week. A key inclusion criterion was borderline zinc deficiency, defined by serum zinc levels in the range of 60–70 µg/dL, as this range indicates a risk for metabolic dysfunctions while not necessitating immediate medical intervention for severe deficiency [1010Nadruz W Jr, Bellinazzi VR, Carvalheira JB. Zinc deficiency leading to intractable Arch Intern Med. 2002 Nov 11;162(20):2376-7. doi: 10.1001/archinte.162.20.2376. PMID: 12418953.]. Zinc deficiency is particularly common in children from low-income settings due to diets high in phytates and low in bioavailable zinc, as well as limited intake of animal-based protein [1111Aggett IP zinc In: Annales Nestleù of Institute Food Research Park, United Kingdom 1994; 52: 94-106.,1212Yamaguchi H, Arita Y, Hara Y, Kimura T, Nawata H. Anorexia nervosa responding to zinc supplementation: a case report. Gastroenterol Jpn. 1992 Aug;27(4):554-8. doi: 10.1007/BF02777794. PMID: 1526438.].
On day 0 of the study, the children were assessed for vomiting duration, anorexia, and nutritional status using weight-for-age Z scores (WAZ) and height-for-age Z scores (HAZ), based on the growth reference data from the National Center for Health Statistics (NCHS) of the USA [44Namakin K, Sharifzadeh GR, Zardast M, Khoshmohabbat Z, Saboori M. Comparison of the WHO Child Growth Standards with the NCHS for Estimation of Malnutrition in Birjand-Iran. Int J Prev Med. 2014 May;5(5):653-7. PMID: 24932399; PMCID: PMC4050688.]. Length (for children under 24 months) or standing height (for children over 24 months) and weight were measured by the same individual. Length and height were recorded in centimeters using an infant meter, while weight was recorded in kilograms using a pediatric scale. Height was measured on day 0, and weight was measured on days 0 and 30.
Sample size and rationale:The sample size was determined based on the prevalence of zinc deficiency in the target population and the anticipated effects of supplementation on vomiting cessation. The limited sample size was due to logistical constraints but was sufficient for statistical validity. Borderline zinc-deficient children were identified using serum zinc levels (<70 mg/dL).
Anorexia: For quality, the child had manifestations of eating and sucking refusal; for quantity, food intake was decreased compared with the one before [55Bryant-Waugh R, Markham L, Kreipe RE, Walsh BT. Feeding and eating disorders in childhood. Int J Eat Disord. 2010 Mar;43(2):98-111. doi: 10.1002/eat.20795. PMID: 20063374.].
Sleep disorders:These include difficulty falling asleep, frequent awakenings (≥ 3 times per night), insomnia, crying at night, and a reduction in total sleep duration compared to normal previous sleep patterns [66Jha VM, Jha SK. Sleep: Disorders and Clinical Implications. In: Sleep: Evolution and Functions. Springer, Singapore. Sleep: Evolution and Functions. 2020;101-118. https://doi.org/10.1007/978-981-15-7175-6_6.].
Diagnosis of zinc deficiency in children:Zinc deficiency is diagnosed when serum zinc concentration is below 70 mg/dL [77International Zinc Nutrition Consultative Group (IZiNCG); Brown KH, Rivera JA, Bhutta Z, Gibson RS, King JC, Lönnerdal B, Ruel MT, Sandtröm B, Wasantwisut E, Hotz C. International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr Bull. 2004 Mar;25(1 Suppl 2):S99-203. PMID: 18046856.].
Energy intake:The energy intake of the subjects was estimated using the twenty-four-hour recall method over three consecutive days [88Somji SS, Dhingra P, Dhingra U, Dutta A, Devi P, Kumar J, Deb S, Semwal OP, Sazawal S, Manji K, Kisenge R, Bakari M, Aboud S, Liu E, Sudfeld C, Duggan CP, Ashorn P, Bahl R, Simon JL. Effect of dose reduction of supplemental zinc for childhood diarrhoea: study protocol for a double-masked, randomised controlled trial in India and Tanzania. BMJ Paediatr Open. 2019 Apr 24;3(1):e000460. doi: 10.1136/bmjpo-2019-000460. Erratum in: BMJ Paediatr Open. 2020 Oct 12;4(1):e000460corr1. doi: 10.1136/bmjpo-2019-000460corr1. PMID: 31206083; PMCID: PMC6542451.]. Standard measuring tableware items, such as bowls, plates, glasses, spoons, and feeding bottles of various sizes, were used to assist mothers in accurately describing the quantity of food consumed by the child, excluding any portions that were vomited. Breast milk intake was estimated based on the excretory quantity of milk in breastfeeding mothers in Vietnam and other developing countries [1313Minh LHN, Tawfik GM, Ghozy S, Hashan MR, Nam NH, Linh LK, Abdelrahman SAM, Quynh TTH, Khoi Quan N, Nhat Le T, Ibrahim HY, El-Nile MO, Kamel AMA, Giang HTN, Huy NT. Feto-Maternal Outcomes of Breastfeeding during Pregnancy: A Systematic Review and Meta-Analysis. J Trop Pediatr. 2021 Dec 8;67(6):fmab097. doi: 10.1093/tropej/fmab097. PMID: 34962568.]. Foods were converted into their raw, uncooked equivalents, and the energy values were calculated using the "A Food Products in Vietnam Composition and Nutritive Value Table" [1414Nguyen-Anh D, Umberger WJ, Zeng D. Understanding Vietnamese Urban Consumers' Nutrition Label Use, Health Concerns, and Consumption of Food and Beverages with Added Sugars. Nutrients. 2020 Oct 29;12(11):3335. doi: 10.3390/nu12113335. PMID: 33138339; PMCID: PMC7694047.].
Enzymatic activity as a marker
Zinc is a cofactor in over 300 enzymes critical to various metabolic pathways. In this study, the following zinc-dependent enzymes were used as biomarkers to validate the intervention:
- Alkaline phosphatase (ALP): Facilitates dephosphory-lation, critical in bone metabolism and cellular regulation.
- Carbonic anhydrase: Regulates pH balance and influences digestive function.
The baseline and post-intervention activities of these enzymes were assessed to confirm the physiological impact of zinc supplementation.
Design
The subjects were randomly assigned to two groups: a supplemented group (S group) that received an oral dose of 10 mg/child of elemental zinc daily, along with iron and vitamins in supplemental dosages, and a non-supplemented group (NS group) that received a similar regimen but without zinc. Vomiting was assessed on days 7, 10, and 15. Serum zinc levels were measured on days 0 and 90. Anthropometric measures (weight gain and energy intake) were recorded on days 0 and 30. Throughout the study, all children were monitored by one physician and two nurses, and they were re-examined on days 7, 10, and 15, as well as monthly and whenever unexpected illness occurred. The research protocol applied from the Department of Pediatrics, University of Medicine and Pharmacy, as well as the Rehabilitation Center for Malnourished Children and Support for Handicapped Children. All measurements were conducted using standardized procedures to ensure consistency.
Rationale for zinc dosage: The study administered 10 mg of elemental zinc per day in the form of zinc gluconate. This dosage was selected based on established safe and effective levels for young children with borderline deficiency, as it optimizes serum zinc restoration while minimizing potential side effects like nausea or gastrointestinal upset [1515Maret W. Zinc biochemistry: from a single zinc enzyme to a key element of life. Adv Nutr. 2013 Jan 1;4(1):82-91. doi: 10.3945/an.112.003038. PMID: 23319127; PMCID: PMC3648744.]. The supplementation period lasted 90 days to allow for observable changes in both enzymatic activity and clinical outcomes.
Supplementation
The zinc-treated subjects (S group) received a daily supplement of 10 mg of elemental zinc in the form of gluconate, along with iron and vitamins at supplemental dosages. The control subjects (NS group) received a similar supplement, minus the zinc, over 90 consecutive days. The supplements were prepared as powdered forms mixed with sugar and packaged into two types of packets: "B" containing zinc and "A" without zinc. Mothers were instructed to add a small amount of water to the powder before administration.
Supplement Composition
The zinc supplement contained:
- Zinc (10 mg/child/day as gluconate): Essential for enzymatic and immune functions.
- Iron (5 mg): To address coexisting risks of iron deficiency anemia.
- Vitamin A (400 IU): Enhances epithelial integrity and immune responses.
- Vitamin C (20 mg): Promotes zinc absorption and provides antioxidant protection.
- Vitamin B complex (B6 and B12): Supports energy metabolism and neurological health.
The multi-micronutrient approach aimed to address common nutritional deficiencies without confounding the specific effect of zinc on vomiting.
Serum zinc measurement
Serum zinc levels were measured in all children at the beginning of the study and on day 60 using differential pulse polarography with stripping. This method is noted for its accuracy, high sensitivity, and selectivity, and it allows for the detection of elements in small serum samples (0.5 - 1 ml) using the 746 VA Trace Analyzer from Metrohm Ltd., CH-9101 Herisau, Switzerland. Serum samples were obtained by centrifuging 1 ml of serum from 3 ml of blood drawn from a peripheral vein. The serum samples were then stored at -20 °C until they were analyzed by the Department of Analytical Chemistry, University of Natural Sciences.
Statistical analysis
The mean ± standard deviation (s.d.) of WAZ (weight-for-age Z-score), HAZ (height-for-age Z-score), vomiting duration (in months), and vomiting frequency (per day) were calculated on day 0. The percentage of vomiting cessation in both groups was assessed using a t-test for two proportions on days 7, 10, and 15. A sign test was used to compare pre- and post-supplementation values within the S group after 7 days. A Student's t-test was employed to compare the mean ± s.d. of energy intake and weight gain between the two groups on day 30, and serum zinc levels were assessed on day 90. A p-value of < 0.05 was considered statistically significant. Statistical analysis was performed on an IBM-compatible computer using the Epi Info version 6.0 program.
Ethical approval
The study was conducted under the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of the Rehabilitation Center for Malnourished Children and Support for Handicapped Children (No. 0129/CMS-HĐYĐ) before official data collection. All study participants provided written informed consent, and their information was kept confidential and solely used for research purposes.
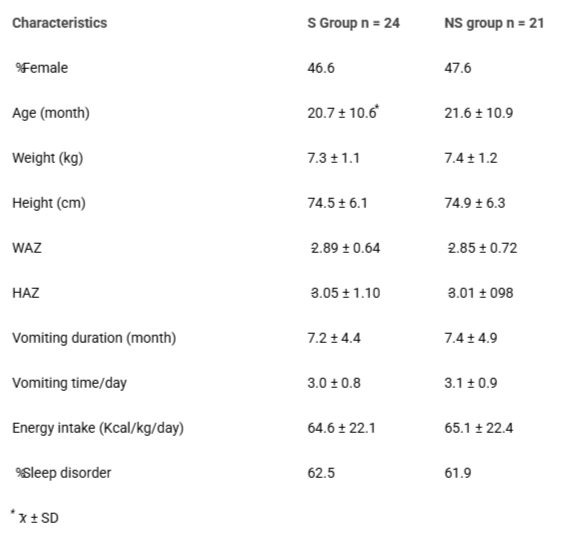
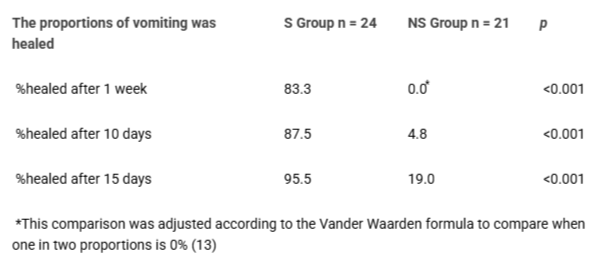
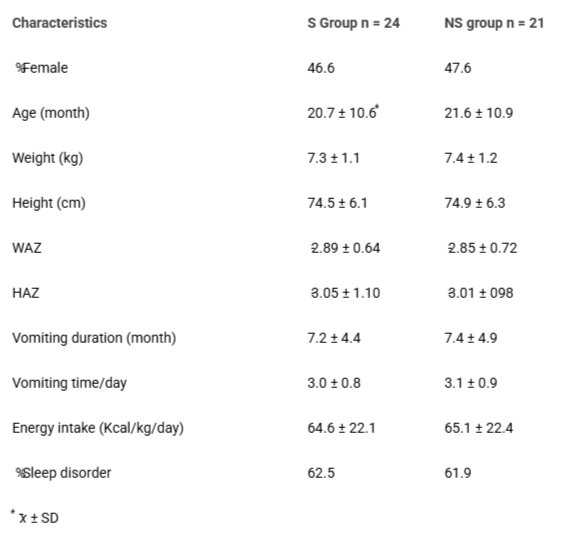
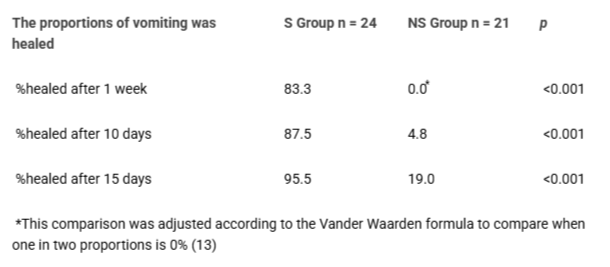
Forty-five subjects completed the study, while five subjects withdrew for various reasons: two families moved to other provinces (one from the S group and one from the NS group), and three parents in the NS group voluntarily withdrew their children, believing that the vomiting had decreased. On day 0, there were no significant differences between the zinc group and the control group regarding the study variables. The mean ± SD of the anthropometric indices, energy intake, and serum zinc levels were low, indicating malnutrition among the subjects. Additionally, the mean ± SD duration of vomiting was prolonged in both groups. Zinc deficiency was present in 71% of the subjects. Furthermore, the subjects exhibited symptoms of jitteriness and sleep disorders (Table 1). On days 7, 10, and 15, the proportions of subjects with resolved vomiting were significantly higher in the S group compared to the NS group (83.3% vs. 0.0%, 87.5% vs. 4.8%, 95.5% vs. 19.0%, respectively, p < 0.001 for each; Table 2).
Table 1: Characteristics of the study group on admission.
Table 2: The healed effect of zinc supplementation on vomiting.
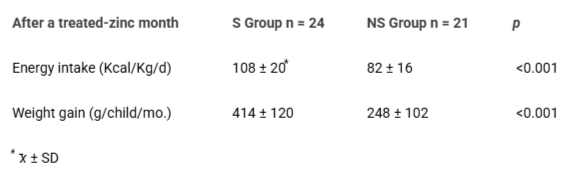
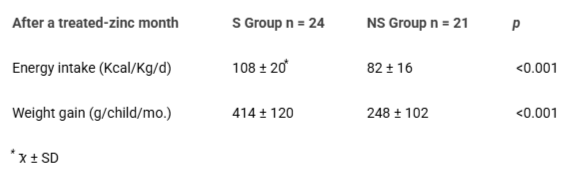
A comparison before and after 7 days of zinc supplementation in the zinc-treated subjects, using the sign test, demonstrated that zinc supplementation had a significant effect on 88% of vomiting cases (with 83% of cases fully healed and 5% showing a decrease in symptoms), reaching a 99% confidence level. In contrast, no changes (0%) were observed in the control group during the same period. During the treatment process, three cases of vomiting recurred due to respiratory infections, but these resolved once the infections were treated. After three months, 10 children in the Non-Supplemented (NS) group still experienced vomiting, which was resolved after 12 days of zinc supplementation. On day 30, the mean ± standard deviation of energy intake (108 ± 20 vs. 82 ± 16, p < 0.001) and weight gain (414 ± 120 vs. 248 ± 102, p < 0.001) in the zinc-supplemented (S) group were significantly higher than in the NS group (Table 3).
Table 3: Effect of zinc supplementation on energy intake and weight gain.
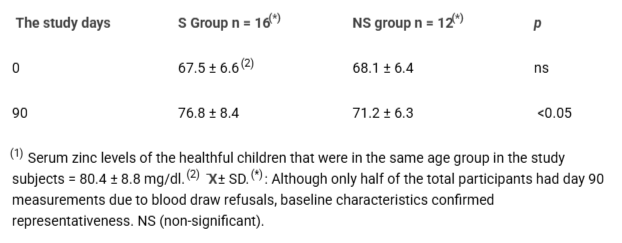
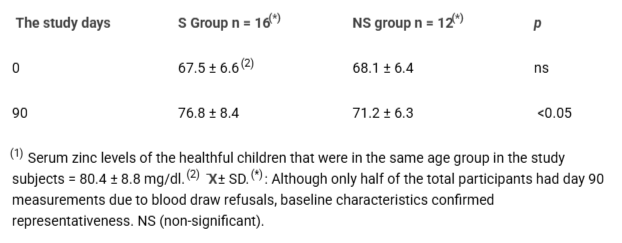
In the final study, due to psychological concerns among some parents about their children losing blood, seventeen mothers refused to have their child’s blood drawn a second time. However, the initial characteristics of the children, regardless of whether their zinc levels were measured at the second time point, did not differ significantly. On day 90, the serum zinc levels of the remaining participants in the S group were significantly higher than those in the NS group (76.8 ± 8.4 vs. 71.2 ± 6.3 mg/dl, p < 0.05) (Table 4).
Table 4: Effect of zinc supplementation on serum levels (μg/dl)(1).
The study results showed that zinc supplementation not only improved food intake and weight gain among the subjects, consistent with the findings of previous studies [1616Abdollahi M, Ajami M, Abdollahi Z, Kalantari N, Houshiarrad A, Fozouni F, Fallahrokni A, Mazandarani FS. Zinc supplementation is an effective and feasible strategy to prevent growth retardation in 6 to 24 month children: A pragmatic double blind, randomized trial. Heliyon. 2019 Nov 1;5(11):e02581. doi: 10.1016/j.heliyon.2019.e02581. PMID: 31720482; PMCID: PMC6839004.-1818Golden MH, Golden BE. Effect of zinc supplementation on the dietary intake, rate of weight gain, and energy cost of tissue deposition in children recovering from severe malnutrition. Am J Clin Nutr. 1981 May;34(5):900-8. doi: 10.1093/ajcn/34.5.900. PMID: 6786072.] but also alleviated vomiting. The subjects whose serum zinc levels were measured were representative of the entire study group, suggesting that the observed changes in zinc levels could be generalized to the whole group. Although the final serum zinc levels of the subjects returned to the normal range, they were slightly lower than those reported in other studies [1919Castillo-Duran C, Heresi G, Fisberg M, Uauy R. Controlled trial of zinc supplementation during recovery from malnutrition: effects on growth and immune function. Am J Clin Nutr. 1987 Mar;45(3):602-8. doi: 10.1093/ajcn/45.3.602. PMID: 3103416.-2121Moran VH, Stammers AL, Medina MW, Patel S, Dykes F, Souverein OW, Dullemeijer C, Pérez-Rodrigo C, Serra-Majem L, Nissensohn M, Lowe NM. The relationship between zinc intake and serum/plasma zinc concentration in children: a systematic review and dose-response meta-analysis. Nutrients. 2012 Aug;4(8):841-58. doi: 10.3390/nu4080841. Epub 2012 Jul 26. PMID: 23016120; PMCID: PMC3448075.], possibly due to the initially low serum zinc levels in our subjects. Additionally, zinc deficiency in the subjects was likely a contributing factor to the anorexia and decreased energy intake observed [2222Tuormaa TE. Adverse effects of zinc deficiency: a review from the literature. Journal of orthomolecular medicine. 1995;10:149-164.,2323Shay NF, Mangian HF. Neurobiology of zinc-influenced eating behavior. J Nutr. 2000 May;130(5S Suppl):1493S-9S. doi: 10.1093/jn/130.5.1493S. PMID: 10801965.].
Additionally, most of the subjects in this study belong to poor families, similar to the majority of children in the Vietnamese countryside, where they lack adequate breastfeeding [2424Ninh NX, Thissen JP, Collette L, Gerard G, Khoi HH, Ketelslegers JM. Zinc supplementation increases growth and circulating insulin-like growth factor I (IGF-I) in growth-retarded Vietnamese children. Am J Clin Nutr. 1996 Apr;63(4):514-9. doi: 10.1093/ajcn/63.4.514. PMID: 8599314.-2626Nguyen HT, Eriksson B, Petzold M, Bondjers G, Tran TK, Nguyen LT, Ascher H. Factors associated with physical growth of children during the first two years of life in rural and urban areas of Vietnam. BMC Pediatr. 2013 Sep 25;13:149. doi: 10.1186/1471-2431-13-149. PMID: 24066791; PMCID: PMC3849555.]. This issue is compounded by the consumption of supplementary foods that are low in energy and animal protein, the latter being a primary source of zinc. Furthermore, the high intake of rice and vegetables, which are rich in phytates and fibers, can hinder zinc absorption and is consistent with the presence of infectious diseases [2727Chau TTN. Promotion of the consumption of local foods to improve the diet of Vietnamese children (Doctoral dissertation, Ghent University, Faculty of Bioscience Engineering). 2016.,2828Huong le T, Xuan le TT, Phuong le H, Huyen DT, Rocklöv J. Diet and nutritional status among children 24-59 months by seasons in a mountainous area of Northern Vietnam in 2012. Glob Health Action. 2014 Dec 8;7:23121. doi: 10.3402/gha.v7.23121. PMID: 25511885; PMCID: PMC4265645.]. The findings suggest that zinc supplementation is necessary for these subjects. Although our observations indicated that zinc supplementation alleviated vomiting, the underlying mechanism remains unclear. However, considering zinc's biological functions, it is plausible that the vomiting observed may be linked to zinc deficiency, potentially related to the jitteriness symptom of zinc deficiency [1010Nadruz W Jr, Bellinazzi VR, Carvalheira JB. Zinc deficiency leading to intractable Arch Intern Med. 2002 Nov 11;162(20):2376-7. doi: 10.1001/archinte.162.20.2376. PMID: 12418953.,1111Aggett IP zinc In: Annales Nestleù of Institute Food Research Park, United Kingdom 1994; 52: 94-106.]. The associated sleep disturbances might also be a manifestation of this deficiency [2929Jazinaki MS, Gheflati A, Moghadam MRSF, Hadi S, Razavidarmian M, Nezhad MY, Akhtari H, Nematizadeh M, Safarian M. Effects of zinc supplementation on sleep quality in humans: A systematic review of randomized controlled trials. Health Sci Rep. 2024 Oct 6;7(10):e70019. doi: 10.1002/hsr2.70019. PMID: 39377022; PMCID: PMC11456512.].
Zinc is involved in the activity of over 300 enzymes essential for various metabolic processes, including crucial peptidases in the digestive tract and enzymes necessary for protein synthesis, where zinc acts as a catalyst [3030Harris ED. Inorganic cofactors. In: Encyclopedia of human nutrition. Vol. I, Academic Press, San Diego 1999; 419-423.-3131Prasad AS. Zinc in human health: effect of zinc on immune cells. Mol Med. 2008 May-Jun;14(5-6):353-7. doi: 10.2119/2008-00033.Prasad. PMID: 18385818; PMCID: PMC2277319.]. Additionally, zinc influences the activity of important hormones involved in metabolism, such as insulin, growth hormone, thyroxin, testosterone, and insulin-like growth factor-1 [1515Maret W. Zinc biochemistry: from a single zinc enzyme to a key element of life. Adv Nutr. 2013 Jan 1;4(1):82-91. doi: 10.3945/an.112.003038. PMID: 23319127; PMCID: PMC3648744.,3232Vallee BL, Auld DS. Zinc coordination, function, and structure of zinc enzymes and other proteins. Biochemistry. 1990 Jun 19;29(24):5647-59. doi: 10.1021/bi00476a001. PMID: 2200508.,3333Foster M, Samman S. Zinc and regulation of inflammatory cytokines: implications for cardiometabolic disease. Nutrients. 2012 Jul;4(7):676-94. doi: 10.3390/nu4070676. Epub 2012 Jul 4. PMID: 22852057; PMCID: PMC3407988.]. Therefore, zinc deficiency may impair metabolic processes, potentially causing stagnation in the digestive tract due to reduced enzyme activity and influencing the functions of the aforementioned hormones [3434Chasapis CT, Loutsidou AC, Spiliopoulou CA, Stefanidou ME. Zinc and human health: an update. Arch Toxicol. 2012 Apr;86(4):521-34. doi: 10.1007/s00204-011-0775-1. Epub 2011 Nov 10. PMID: 22071549.]. Vomiting in these cases might be a response to relieve stagnation and irritation in the stomach, and it may also be a manifestation of jitteriness in the subjects. The observed improvement in vomiting following zinc supplementation could be due to the reduction of jitteriness and the restoration of enzyme activity [1212Yamaguchi H, Arita Y, Hara Y, Kimura T, Nawata H. Anorexia nervosa responding to zinc supplementation: a case report. Gastroenterol Jpn. 1992 Aug;27(4):554-8. doi: 10.1007/BF02777794. PMID: 1526438.,3535Alam AN, Sarker SA, Wahed MA, Khatun M, Rahaman MM. Enteric protein loss and intestinal permeability changes in children during acute shigellosis and after recovery: effect of zinc supplementation. Gut. 1994 Dec;35(12):1707-11. doi: 10.1136/gut.35.12.1707. PMID: 7829006; PMCID: PMC1375257.]. Previous studies have demonstrated that zinc supplementation can restore the activity of zinc-dependent enzymes, leading to increased absorption of lipids and proteins [3636Golden BE, Golden MH. Effect of zinc on lean tissue synthesis during recovery from malnutrition. Eur J Clin Nutr. 1992 Oct;46(10):697-706. PMID: 1425524.-4040Nguyen CL, Hoang DV, Nguyen PTH, Ha AVV, Chu TK, Pham NM, Lee AH, Duong DV, Binns CW. Low Dietary Intakes of Essential Nutrients during Pregnancy in Vietnam. Nutrients. 2018 Aug 6;10(8):1025. doi: 10.3390/nu10081025. PMID: 30082626; PMCID: PMC6116189. ].
Zinc supplementation improved vomiting, nutritional intake, and weight gain in anorexic children, aligning with prior studies. Zinc’s role in enzyme activity and hormone regulation likely contributed to these outcomes. Despite promising results, the study’s limitations include a small sample size and lack of long-term follow-up. Future research should explore zinc’s toxic effects and investigate optimal dosages.
Limitations and future directions
Limited sample size necessitates caution in generalizing results. Future studies should assess long-term impacts and zinc toxicity at higher doses. Also, investigations into the precise mechanisms of zinc’s effects on vomiting are warranted.
This study demonstrated that zinc supplementation significantly reduces vomiting frequency and improves appetite, energy intake, and weight gain in anorexic children with prolonged vomiting. Zinc's role in restoring enzymatic activity and addressing borderline deficiency highlights its therapeutic potential. We recommend routine zinc supplementation (10 mg/day) for children with similar clinical profiles, particularly in settings with high deficiency prevalence. Future research should explore the long-term effects of zinc on digestive health and its interplay with other micronutrients.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Author contribution statement
D. N. and D. T. N. conceived and designed the evaluation and drafted the manuscript. X. H. D. and P. P. N. participated in designing the evaluation, performed parts of the statistical analysis, and helped to draft the manuscript. T. D. N. re-evaluated the clinical data, revised the manuscript performed the statistical analysis, and revised the manuscript. D. T. N. collected the clinical data, interpreted them, and revised the manuscript. X. H. D. re-analyzed the clinical and statistical data and revised the manuscript. P. P. N. had a critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript.
Ethical declaration: Informed consent was obtained from all subjects involved in the study.
Data availability statement: All the data available is provided in this paper.
Ravindranath A. Chronic vomiting in children: Etiology, diagnosis, and management. Indian J Gastroenterol. 2020 Apr;39(2):117-122. doi: 10.1007/s12664-020-01035-w. PMID: 32385612.
Vomiting in Children: Clinical Scenarios. Current Treatment Options in Pediatrics, 2023; 9(1): 1-14. https://doi.org/10.1007/s40746-023-00283-0.
Namakin K, Sharifzadeh GR, Zardast M, Khoshmohabbat Z, Saboori M. Comparison of the WHO Child Growth Standards with the NCHS for Estimation of Malnutrition in Birjand-Iran. Int J Prev Med. 2014 May;5(5):653-7. PMID: 24932399; PMCID: PMC4050688.
Bryant-Waugh R, Markham L, Kreipe RE, Walsh BT. Feeding and eating disorders in childhood. Int J Eat Disord. 2010 Mar;43(2):98-111. doi: 10.1002/eat.20795. PMID: 20063374.
Jha VM, Jha SK. Sleep: Disorders and Clinical Implications. In: Sleep: Evolution and Functions. Springer, Singapore. Sleep: Evolution and Functions. 2020;101-118. https://doi.org/10.1007/978-981-15-7175-6_6.
International Zinc Nutrition Consultative Group (IZiNCG); Brown KH, Rivera JA, Bhutta Z, Gibson RS, King JC, Lönnerdal B, Ruel MT, Sandtröm B, Wasantwisut E, Hotz C. International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr Bull. 2004 Mar;25(1 Suppl 2):S99-203. PMID: 18046856.
Somji SS, Dhingra P, Dhingra U, Dutta A, Devi P, Kumar J, Deb S, Semwal OP, Sazawal S, Manji K, Kisenge R, Bakari M, Aboud S, Liu E, Sudfeld C, Duggan CP, Ashorn P, Bahl R, Simon JL. Effect of dose reduction of supplemental zinc for childhood diarrhoea: study protocol for a double-masked, randomised controlled trial in India and Tanzania. BMJ Paediatr Open. 2019 Apr 24;3(1):e000460. doi: 10.1136/bmjpo-2019-000460. Erratum in: BMJ Paediatr Open. 2020 Oct 12;4(1):e000460corr1. doi: 10.1136/bmjpo-2019-000460corr1. PMID: 31206083; PMCID: PMC6542451.
Dewey KG, Brown KH. Update on technical issues concerning complementary feeding of young children in developing countries and implications for intervention programs. Food Nutr Bull. 2003 Mar;24(1):5-28. doi: 10.1177/156482650302400102. Erratum in: Food Nutr Bull. 2003 Jun;24(2):239. PMID: 12664525.
Nadruz W Jr, Bellinazzi VR, Carvalheira JB. Zinc deficiency leading to intractable Arch Intern Med. 2002 Nov 11;162(20):2376-7. doi: 10.1001/archinte.162.20.2376. PMID: 12418953.
Aggett IP zinc In: Annales Nestleù of Institute Food Research Park, United Kingdom 1994; 52: 94-106.
Yamaguchi H, Arita Y, Hara Y, Kimura T, Nawata H. Anorexia nervosa responding to zinc supplementation: a case report. Gastroenterol Jpn. 1992 Aug;27(4):554-8. doi: 10.1007/BF02777794. PMID: 1526438.
Minh LHN, Tawfik GM, Ghozy S, Hashan MR, Nam NH, Linh LK, Abdelrahman SAM, Quynh TTH, Khoi Quan N, Nhat Le T, Ibrahim HY, El-Nile MO, Kamel AMA, Giang HTN, Huy NT. Feto-Maternal Outcomes of Breastfeeding during Pregnancy: A Systematic Review and Meta-Analysis. J Trop Pediatr. 2021 Dec 8;67(6):fmab097. doi: 10.1093/tropej/fmab097. PMID: 34962568.
Nguyen-Anh D, Umberger WJ, Zeng D. Understanding Vietnamese Urban Consumers' Nutrition Label Use, Health Concerns, and Consumption of Food and Beverages with Added Sugars. Nutrients. 2020 Oct 29;12(11):3335. doi: 10.3390/nu12113335. PMID: 33138339; PMCID: PMC7694047.
Maret W. Zinc biochemistry: from a single zinc enzyme to a key element of life. Adv Nutr. 2013 Jan 1;4(1):82-91. doi: 10.3945/an.112.003038. PMID: 23319127; PMCID: PMC3648744.
Abdollahi M, Ajami M, Abdollahi Z, Kalantari N, Houshiarrad A, Fozouni F, Fallahrokni A, Mazandarani FS. Zinc supplementation is an effective and feasible strategy to prevent growth retardation in 6 to 24 month children: A pragmatic double blind, randomized trial. Heliyon. 2019 Nov 1;5(11):e02581. doi: 10.1016/j.heliyon.2019.e02581. PMID: 31720482; PMCID: PMC6839004.
Mozaffari-Khosravi H, Shakiba M, Eftekhari MH, Fatehi F. Effects of zinc supplementation on physical growth in 2-5-year-old children. Biol Trace Elem Res. 2009 May;128(2):118-27. doi: 10.1007/s12011-008-8261-1. Epub 2008 Oct 28. PMID: 18956153.
Golden MH, Golden BE. Effect of zinc supplementation on the dietary intake, rate of weight gain, and energy cost of tissue deposition in children recovering from severe malnutrition. Am J Clin Nutr. 1981 May;34(5):900-8. doi: 10.1093/ajcn/34.5.900. PMID: 6786072.
Castillo-Duran C, Heresi G, Fisberg M, Uauy R. Controlled trial of zinc supplementation during recovery from malnutrition: effects on growth and immune function. Am J Clin Nutr. 1987 Mar;45(3):602-8. doi: 10.1093/ajcn/45.3.602. PMID: 3103416.
Simmer K, Khanum S, Carlsson L, Thompson RP. Nutritional rehabilitation in Bangladesh--the importance of zinc. Am J Clin Nutr. 1988 Jun;47(6):1036-40. doi: 10.1093/ajcn/47.6.1036. PMID: 3132034.
Moran VH, Stammers AL, Medina MW, Patel S, Dykes F, Souverein OW, Dullemeijer C, Pérez-Rodrigo C, Serra-Majem L, Nissensohn M, Lowe NM. The relationship between zinc intake and serum/plasma zinc concentration in children: a systematic review and dose-response meta-analysis. Nutrients. 2012 Aug;4(8):841-58. doi: 10.3390/nu4080841. Epub 2012 Jul 26. PMID: 23016120; PMCID: PMC3448075.
Tuormaa TE. Adverse effects of zinc deficiency: a review from the literature. Journal of orthomolecular medicine. 1995;10:149-164.
Ninh NX, Thissen JP, Collette L, Gerard G, Khoi HH, Ketelslegers JM. Zinc supplementation increases growth and circulating insulin-like growth factor I (IGF-I) in growth-retarded Vietnamese children. Am J Clin Nutr. 1996 Apr;63(4):514-9. doi: 10.1093/ajcn/63.4.514. PMID: 8599314.
Tuan NT, Nguyen PH, Hajeebhoy N, Frongillo EA. Gaps between breastfeeding awareness and practices in Vietnamese mothers result from inadequate support in health facilities and social norms. J Nutr. 2014 Nov;144(11):1811-7. doi: 10.3945/jn.114.198226. Epub 2014 Sep 3. PMID: 25332480.
Nguyen HT, Eriksson B, Petzold M, Bondjers G, Tran TK, Nguyen LT, Ascher H. Factors associated with physical growth of children during the first two years of life in rural and urban areas of Vietnam. BMC Pediatr. 2013 Sep 25;13:149. doi: 10.1186/1471-2431-13-149. PMID: 24066791; PMCID: PMC3849555.
Chau TTN. Promotion of the consumption of local foods to improve the diet of Vietnamese children (Doctoral dissertation, Ghent University, Faculty of Bioscience Engineering). 2016.
Huong le T, Xuan le TT, Phuong le H, Huyen DT, Rocklöv J. Diet and nutritional status among children 24-59 months by seasons in a mountainous area of Northern Vietnam in 2012. Glob Health Action. 2014 Dec 8;7:23121. doi: 10.3402/gha.v7.23121. PMID: 25511885; PMCID: PMC4265645.
Jazinaki MS, Gheflati A, Moghadam MRSF, Hadi S, Razavidarmian M, Nezhad MY, Akhtari H, Nematizadeh M, Safarian M. Effects of zinc supplementation on sleep quality in humans: A systematic review of randomized controlled trials. Health Sci Rep. 2024 Oct 6;7(10):e70019. doi: 10.1002/hsr2.70019. PMID: 39377022; PMCID: PMC11456512.
Harris ED. Inorganic cofactors. In: Encyclopedia of human nutrition. Vol. I, Academic Press, San Diego 1999; 419-423.
Prasad AS. Zinc in human health: effect of zinc on immune cells. Mol Med. 2008 May-Jun;14(5-6):353-7. doi: 10.2119/2008-00033.Prasad. PMID: 18385818; PMCID: PMC2277319.
Vallee BL, Auld DS. Zinc coordination, function, and structure of zinc enzymes and other proteins. Biochemistry. 1990 Jun 19;29(24):5647-59. doi: 10.1021/bi00476a001. PMID: 2200508.
Foster M, Samman S. Zinc and regulation of inflammatory cytokines: implications for cardiometabolic disease. Nutrients. 2012 Jul;4(7):676-94. doi: 10.3390/nu4070676. Epub 2012 Jul 4. PMID: 22852057; PMCID: PMC3407988.
Chasapis CT, Loutsidou AC, Spiliopoulou CA, Stefanidou ME. Zinc and human health: an update. Arch Toxicol. 2012 Apr;86(4):521-34. doi: 10.1007/s00204-011-0775-1. Epub 2011 Nov 10. PMID: 22071549.
Alam AN, Sarker SA, Wahed MA, Khatun M, Rahaman MM. Enteric protein loss and intestinal permeability changes in children during acute shigellosis and after recovery: effect of zinc supplementation. Gut. 1994 Dec;35(12):1707-11. doi: 10.1136/gut.35.12.1707. PMID: 7829006; PMCID: PMC1375257.
Golden BE, Golden MH. Effect of zinc on lean tissue synthesis during recovery from malnutrition. Eur J Clin Nutr. 1992 Oct;46(10):697-706. PMID: 1425524.
Wessels I, Fischer HJ, Rink L. Dietary and Physiological Effects of Zinc on the Immune System. Annu Rev Nutr. 2021 Oct 11;41:133-175. doi: 10.1146/annurev-nutr-122019-120635. Epub 2021 Jul 13. PMID: 34255547.
Chasapis CT, Ntoupa PA, Spiliopoulou CA, Stefanidou ME. Recent aspects of the effects of zinc on human health. Arch Toxicol. 2020 May;94(5):1443-1460. doi: 10.1007/s00204-020-02702-9. Epub 2020 May 12. PMID: 32394086.
Ramakrishnan U, Goldenberg T, Allen LH. Do multiple micronutrient interventions improve child health, growth, and development? J Nutr. 2011 Nov;141(11):2066-75. doi: 10.3945/jn.111.146845. Epub 2011 Sep 28. PMID: 21956959.
Nguyen CL, Hoang DV, Nguyen PTH, Ha AVV, Chu TK, Pham NM, Lee AH, Duong DV, Binns CW. Low Dietary Intakes of Essential Nutrients during Pregnancy in Vietnam. Nutrients. 2018 Aug 6;10(8):1025. doi: 10.3390/nu10081025. PMID: 30082626; PMCID: PMC6116189.
Thai ND, Xuyen DH, Phuong NP, Danh NT. Zinc Supplementation in Anorexic Children with Vomiting Syndrome: Evaluation from a Randomized Controlled Trial in Vietnam. IgMin Res. January 17, 2025; 3(1): 015-020. IgMin ID: igmin279; DOI:10.61927/igmin279; Available at: igmin.link/p279
1General clinic, National Institute for Control of Vaccines and Biologicals, Hanoi City, Vietnam
2Department of Physiology, Vietnam University of Traditional Medicine, Hanoi City, Vietnam
3Clinic of Nutritional Medicine and Pediatrics, Ho Chi Minh City Nutrition Research Institute, Ho Chi Minh, City, Vietnam
Address Correspondence: Thai Nguyen Duy, General clinic, National Institute for Control of Vaccines and Biologicals, Hanoi city, Vietnam, Email: [email protected]; Nguyen Thanh Danh, Clinic of Nutritional Medicine and Pediatrics, Ho Chi Minh City Nutrition Research Institute, Ho Chi Minh, City, Vietnam, Email: [email protected]
How to cite this article: Thai ND, Xuyen DH, Phuong NP, Danh NT. Zinc Supplementation in Anorexic Children with Vomiting Syndrome: Evaluation from a Randomized Controlled Trial in Vietnam. IgMin Res. January 17, 2025; 3(1): 015-020. IgMin ID: igmin279; DOI:10.61927/igmin279; Available at: igmin.link/p279
Table 1: Characteristics of the study group on admission....
Table 2: The healed effect of zinc supplementation on vomit...
Table 3: Effect of zinc supplementation on energy intake an...
Table 4: Effect of zinc supplementation on serum levels (&m...
Ravindranath A. Chronic vomiting in children: Etiology, diagnosis, and management. Indian J Gastroenterol. 2020 Apr;39(2):117-122. doi: 10.1007/s12664-020-01035-w. PMID: 32385612.
Vomiting in Children: Clinical Scenarios. Current Treatment Options in Pediatrics, 2023; 9(1): 1-14. https://doi.org/10.1007/s40746-023-00283-0.
Namakin K, Sharifzadeh GR, Zardast M, Khoshmohabbat Z, Saboori M. Comparison of the WHO Child Growth Standards with the NCHS for Estimation of Malnutrition in Birjand-Iran. Int J Prev Med. 2014 May;5(5):653-7. PMID: 24932399; PMCID: PMC4050688.
Bryant-Waugh R, Markham L, Kreipe RE, Walsh BT. Feeding and eating disorders in childhood. Int J Eat Disord. 2010 Mar;43(2):98-111. doi: 10.1002/eat.20795. PMID: 20063374.
Jha VM, Jha SK. Sleep: Disorders and Clinical Implications. In: Sleep: Evolution and Functions. Springer, Singapore. Sleep: Evolution and Functions. 2020;101-118. https://doi.org/10.1007/978-981-15-7175-6_6.
International Zinc Nutrition Consultative Group (IZiNCG); Brown KH, Rivera JA, Bhutta Z, Gibson RS, King JC, Lönnerdal B, Ruel MT, Sandtröm B, Wasantwisut E, Hotz C. International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr Bull. 2004 Mar;25(1 Suppl 2):S99-203. PMID: 18046856.
Somji SS, Dhingra P, Dhingra U, Dutta A, Devi P, Kumar J, Deb S, Semwal OP, Sazawal S, Manji K, Kisenge R, Bakari M, Aboud S, Liu E, Sudfeld C, Duggan CP, Ashorn P, Bahl R, Simon JL. Effect of dose reduction of supplemental zinc for childhood diarrhoea: study protocol for a double-masked, randomised controlled trial in India and Tanzania. BMJ Paediatr Open. 2019 Apr 24;3(1):e000460. doi: 10.1136/bmjpo-2019-000460. Erratum in: BMJ Paediatr Open. 2020 Oct 12;4(1):e000460corr1. doi: 10.1136/bmjpo-2019-000460corr1. PMID: 31206083; PMCID: PMC6542451.
Dewey KG, Brown KH. Update on technical issues concerning complementary feeding of young children in developing countries and implications for intervention programs. Food Nutr Bull. 2003 Mar;24(1):5-28. doi: 10.1177/156482650302400102. Erratum in: Food Nutr Bull. 2003 Jun;24(2):239. PMID: 12664525.
Nadruz W Jr, Bellinazzi VR, Carvalheira JB. Zinc deficiency leading to intractable Arch Intern Med. 2002 Nov 11;162(20):2376-7. doi: 10.1001/archinte.162.20.2376. PMID: 12418953.
Aggett IP zinc In: Annales Nestleù of Institute Food Research Park, United Kingdom 1994; 52: 94-106.
Yamaguchi H, Arita Y, Hara Y, Kimura T, Nawata H. Anorexia nervosa responding to zinc supplementation: a case report. Gastroenterol Jpn. 1992 Aug;27(4):554-8. doi: 10.1007/BF02777794. PMID: 1526438.
Minh LHN, Tawfik GM, Ghozy S, Hashan MR, Nam NH, Linh LK, Abdelrahman SAM, Quynh TTH, Khoi Quan N, Nhat Le T, Ibrahim HY, El-Nile MO, Kamel AMA, Giang HTN, Huy NT. Feto-Maternal Outcomes of Breastfeeding during Pregnancy: A Systematic Review and Meta-Analysis. J Trop Pediatr. 2021 Dec 8;67(6):fmab097. doi: 10.1093/tropej/fmab097. PMID: 34962568.
Nguyen-Anh D, Umberger WJ, Zeng D. Understanding Vietnamese Urban Consumers' Nutrition Label Use, Health Concerns, and Consumption of Food and Beverages with Added Sugars. Nutrients. 2020 Oct 29;12(11):3335. doi: 10.3390/nu12113335. PMID: 33138339; PMCID: PMC7694047.
Maret W. Zinc biochemistry: from a single zinc enzyme to a key element of life. Adv Nutr. 2013 Jan 1;4(1):82-91. doi: 10.3945/an.112.003038. PMID: 23319127; PMCID: PMC3648744.
Abdollahi M, Ajami M, Abdollahi Z, Kalantari N, Houshiarrad A, Fozouni F, Fallahrokni A, Mazandarani FS. Zinc supplementation is an effective and feasible strategy to prevent growth retardation in 6 to 24 month children: A pragmatic double blind, randomized trial. Heliyon. 2019 Nov 1;5(11):e02581. doi: 10.1016/j.heliyon.2019.e02581. PMID: 31720482; PMCID: PMC6839004.
Mozaffari-Khosravi H, Shakiba M, Eftekhari MH, Fatehi F. Effects of zinc supplementation on physical growth in 2-5-year-old children. Biol Trace Elem Res. 2009 May;128(2):118-27. doi: 10.1007/s12011-008-8261-1. Epub 2008 Oct 28. PMID: 18956153.
Golden MH, Golden BE. Effect of zinc supplementation on the dietary intake, rate of weight gain, and energy cost of tissue deposition in children recovering from severe malnutrition. Am J Clin Nutr. 1981 May;34(5):900-8. doi: 10.1093/ajcn/34.5.900. PMID: 6786072.
Castillo-Duran C, Heresi G, Fisberg M, Uauy R. Controlled trial of zinc supplementation during recovery from malnutrition: effects on growth and immune function. Am J Clin Nutr. 1987 Mar;45(3):602-8. doi: 10.1093/ajcn/45.3.602. PMID: 3103416.
Simmer K, Khanum S, Carlsson L, Thompson RP. Nutritional rehabilitation in Bangladesh--the importance of zinc. Am J Clin Nutr. 1988 Jun;47(6):1036-40. doi: 10.1093/ajcn/47.6.1036. PMID: 3132034.
Moran VH, Stammers AL, Medina MW, Patel S, Dykes F, Souverein OW, Dullemeijer C, Pérez-Rodrigo C, Serra-Majem L, Nissensohn M, Lowe NM. The relationship between zinc intake and serum/plasma zinc concentration in children: a systematic review and dose-response meta-analysis. Nutrients. 2012 Aug;4(8):841-58. doi: 10.3390/nu4080841. Epub 2012 Jul 26. PMID: 23016120; PMCID: PMC3448075.
Tuormaa TE. Adverse effects of zinc deficiency: a review from the literature. Journal of orthomolecular medicine. 1995;10:149-164.
Ninh NX, Thissen JP, Collette L, Gerard G, Khoi HH, Ketelslegers JM. Zinc supplementation increases growth and circulating insulin-like growth factor I (IGF-I) in growth-retarded Vietnamese children. Am J Clin Nutr. 1996 Apr;63(4):514-9. doi: 10.1093/ajcn/63.4.514. PMID: 8599314.
Tuan NT, Nguyen PH, Hajeebhoy N, Frongillo EA. Gaps between breastfeeding awareness and practices in Vietnamese mothers result from inadequate support in health facilities and social norms. J Nutr. 2014 Nov;144(11):1811-7. doi: 10.3945/jn.114.198226. Epub 2014 Sep 3. PMID: 25332480.
Nguyen HT, Eriksson B, Petzold M, Bondjers G, Tran TK, Nguyen LT, Ascher H. Factors associated with physical growth of children during the first two years of life in rural and urban areas of Vietnam. BMC Pediatr. 2013 Sep 25;13:149. doi: 10.1186/1471-2431-13-149. PMID: 24066791; PMCID: PMC3849555.
Chau TTN. Promotion of the consumption of local foods to improve the diet of Vietnamese children (Doctoral dissertation, Ghent University, Faculty of Bioscience Engineering). 2016.
Huong le T, Xuan le TT, Phuong le H, Huyen DT, Rocklöv J. Diet and nutritional status among children 24-59 months by seasons in a mountainous area of Northern Vietnam in 2012. Glob Health Action. 2014 Dec 8;7:23121. doi: 10.3402/gha.v7.23121. PMID: 25511885; PMCID: PMC4265645.
Jazinaki MS, Gheflati A, Moghadam MRSF, Hadi S, Razavidarmian M, Nezhad MY, Akhtari H, Nematizadeh M, Safarian M. Effects of zinc supplementation on sleep quality in humans: A systematic review of randomized controlled trials. Health Sci Rep. 2024 Oct 6;7(10):e70019. doi: 10.1002/hsr2.70019. PMID: 39377022; PMCID: PMC11456512.
Harris ED. Inorganic cofactors. In: Encyclopedia of human nutrition. Vol. I, Academic Press, San Diego 1999; 419-423.
Prasad AS. Zinc in human health: effect of zinc on immune cells. Mol Med. 2008 May-Jun;14(5-6):353-7. doi: 10.2119/2008-00033.Prasad. PMID: 18385818; PMCID: PMC2277319.
Vallee BL, Auld DS. Zinc coordination, function, and structure of zinc enzymes and other proteins. Biochemistry. 1990 Jun 19;29(24):5647-59. doi: 10.1021/bi00476a001. PMID: 2200508.
Foster M, Samman S. Zinc and regulation of inflammatory cytokines: implications for cardiometabolic disease. Nutrients. 2012 Jul;4(7):676-94. doi: 10.3390/nu4070676. Epub 2012 Jul 4. PMID: 22852057; PMCID: PMC3407988.
Chasapis CT, Loutsidou AC, Spiliopoulou CA, Stefanidou ME. Zinc and human health: an update. Arch Toxicol. 2012 Apr;86(4):521-34. doi: 10.1007/s00204-011-0775-1. Epub 2011 Nov 10. PMID: 22071549.
Alam AN, Sarker SA, Wahed MA, Khatun M, Rahaman MM. Enteric protein loss and intestinal permeability changes in children during acute shigellosis and after recovery: effect of zinc supplementation. Gut. 1994 Dec;35(12):1707-11. doi: 10.1136/gut.35.12.1707. PMID: 7829006; PMCID: PMC1375257.
Golden BE, Golden MH. Effect of zinc on lean tissue synthesis during recovery from malnutrition. Eur J Clin Nutr. 1992 Oct;46(10):697-706. PMID: 1425524.
Wessels I, Fischer HJ, Rink L. Dietary and Physiological Effects of Zinc on the Immune System. Annu Rev Nutr. 2021 Oct 11;41:133-175. doi: 10.1146/annurev-nutr-122019-120635. Epub 2021 Jul 13. PMID: 34255547.
Chasapis CT, Ntoupa PA, Spiliopoulou CA, Stefanidou ME. Recent aspects of the effects of zinc on human health. Arch Toxicol. 2020 May;94(5):1443-1460. doi: 10.1007/s00204-020-02702-9. Epub 2020 May 12. PMID: 32394086.
Ramakrishnan U, Goldenberg T, Allen LH. Do multiple micronutrient interventions improve child health, growth, and development? J Nutr. 2011 Nov;141(11):2066-75. doi: 10.3945/jn.111.146845. Epub 2011 Sep 28. PMID: 21956959.
Nguyen CL, Hoang DV, Nguyen PTH, Ha AVV, Chu TK, Pham NM, Lee AH, Duong DV, Binns CW. Low Dietary Intakes of Essential Nutrients during Pregnancy in Vietnam. Nutrients. 2018 Aug 6;10(8):1025. doi: 10.3390/nu10081025. PMID: 30082626; PMCID: PMC6116189.



 スキャンしてリンクを取得
スキャンしてリンクを取得