Welcome to IgMin Research – an Open Access journal uniting Biology, Medicine, and Engineering. We’re dedicated to advancing global knowledge and fostering collaboration across scientific fields.
Welcome to IgMin, a leading platform dedicated to enhancing knowledge dissemination and professional growth across multiple fields of science, technology, and the humanities. We believe in the power of open access, collaboration, and innovation. Our goal is to provide individuals and organizations with the tools they need to succeed in the global knowledge economy.
IgMin Publications Inc., Suite 102, West Hartford, CT - 06110, USA
Study objective: Adolescent females are disproportionately affected by Sexually Transmitted Infections (STIs). Endocervical Gram stain smears taken during gynecological examination are inexpensive, relatively easy procedures to perform and interpret. The purpose of this study was to evaluate the performance characteristics of Gram smears in the diagnosis of Chlamydia trachomatis (CT), Neisseria gonorrhoeae (GC) and Trichomonas vaginalis (TV)in a female adolescent population presenting to the Emergency Department (ED) with genitourinary complaints.
Methods: This study was a retrospective, cohort analysis of consecutive females (ages 13 – 19) seen at three academic medical centers over a two-year study period. All patients underwent a pelvic exam with diagnostic testing for STIs. Positive criteria for a Gram stain included greater than ten white blood cells per high-power field, gram-negative intracellular/extracellular diplococci (suggesting GC), or direct visualization of TV organisms. Polymerase Chain Reaction (PCR) assays were used as the gold standard definition for CT/GC infection. Direct microscopic visualization of organisms on a separate wet mount prep was considered the gold standard for TV infection. Demographic information, clinical findings of cervicitis, and the results of diagnostic testing were obtained from ED records using standardized abstraction forms.
Results: During the study period, 1303 adolescent females were evaluated for genitourinary complaints. A total of 181 adolescents (12.9%) had at least one documented STI. Overall, 298 patients (22.9%) had positive gram stains. The sensitivity, specificity, and positive likelihood ratio for Gram stain in the diagnosis of STI were 28.7% (95% CI, 22.2 to 35.9), 78.1% (95% CI, 75.5 to 80.5), and 1.31 (95% CI 1.0 to 1.7), respectively. The sensitivity of Gram stain to Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis were 35.9% (95% CI 26.8 to 45.8), 34.5% (95% CI 18.0 to 54.3), and 5.7% (95% CI 1.3 to 15.7), respectively. The consistency of the data recording was excellent, with a median kappa statistic of 0.89.
Conclusions: The positive likelihood ratio of inflammation on endocervical Gram stain is too low to recommend its use to direct empiric treatment of adolescents at risk for sexually transmitted infections. Diagnostic uncertainty or treatment failures should prompt specific laboratory testing.
Adolescents are disproportionately affected by Sexually Transmitted Infections (STIs) including Chlamydia trachomatis (CT), Neisseria gonorrhoeae (GC), and Trichomonas vaginalis (TV). Of approximately 20 million new STIs annually in the United States, half occur among adolescents aged 15–24 years [11Vayngortin T, Gracia M, Clark K, Vayngortin B, Bialostozky M, Heitzman L, Hollenbach K, Kumar M, Titchen K, Bryl A. Increasing Chlamydia and Gonorrhea Testing for Adolescents in the Pediatric Emergency Department. Pediatrics. 2024 Jan 1;153(1):e2022059707. doi: 10.1542/peds.2022-059707. PMID: 38053440; PMCID: PMC11022968.]. It is estimated that one in four sexually active adolescent females has an STI [22Shannon CL, Klausner JD. The growing epidemic of sexually transmitted infections in adolescents: a neglected population. Curr Opin Pediatr. 2018 Feb;30(1):137-143. doi: 10.1097/MOP.0000000000000578. PMID: 29315111; PMCID: PMC5856484.]. STIs can lead to serious health issues, especially when untreated. For example, infections like chlamydia and gonorrhea can cause Pelvic Inflammatory Disease (PID), which may result in infertility or chronic pelvic pain [33Schneider K, FitzGerald M, Byczkowski T, Reed J. Screening for Asymptomatic Gonorrhea and Chlamydia in the Pediatric Emergency Department. Sex Transm Dis. 2016 Apr;43(4):209-15. doi: 10.1097/OLQ.0000000000000424. PMID: 26967296.]. Adolescents are also at higher risk of co-infections with multiple STIs, further complicating health outcomes [44Breslin K, Tuchman L, Hayes KL, Badolato G, Goyal MK. Sensitivity and Specificity of Empiric Treatment for Sexually Transmitted Infections in a Pediatric Emergency Department. J Pediatr. 2017 Oct;189:48-53. doi: 10.1016/j.jpeds.2017.05.050. Epub 2017 Jun 17. PMID: 28629687; PMCID: PMC5614813.]. Despite the substantial impact of STIs on adolescents, most studies and clinical guidelines have historically focused on adult populations [22Shannon CL, Klausner JD. The growing epidemic of sexually transmitted infections in adolescents: a neglected population. Curr Opin Pediatr. 2018 Feb;30(1):137-143. doi: 10.1097/MOP.0000000000000578. PMID: 29315111; PMCID: PMC5856484.]. This is problematic because adolescents have unique needs in terms of prevention, diagnosis, and treatment. For instance, this age group often faces challenges in seeking healthcare due to concerns about confidentiality, cost, and stigma.
Adolescents account for an estimated 15 million Emergency Department (ED) visits annually [44Breslin K, Tuchman L, Hayes KL, Badolato G, Goyal MK. Sensitivity and Specificity of Empiric Treatment for Sexually Transmitted Infections in a Pediatric Emergency Department. J Pediatr. 2017 Oct;189:48-53. doi: 10.1016/j.jpeds.2017.05.050. Epub 2017 Jun 17. PMID: 28629687; PMCID: PMC5614813.]. EDs often act as a primary point of care for many individuals who either lack a primary care physician or are unable to access other health resources for screening, education, or treatment of STIs. This setting is not optimal as suggested by several studies showing both over-treatment and under-treatment of chlamydia and gonorrhea as well as increased costs for testing these diseases in emergency care facilities [22Shannon CL, Klausner JD. The growing epidemic of sexually transmitted infections in adolescents: a neglected population. Curr Opin Pediatr. 2018 Feb;30(1):137-143. doi: 10.1097/MOP.0000000000000578. PMID: 29315111; PMCID: PMC5856484.-55Anaene M, Soyemi K, Caskey R. Factors associated with the over-treatment and under-treatment of gonorrhea and chlamydia in adolescents presenting to a public hospital emergency department. Int J Infect Dis. 2016 Dec;53:34-38. doi: 10.1016/j.ijid.2016.10.009. Epub 2016 Oct 19. PMID: 27771470.]. The reasons for over and under-treatment issues in the ED setting include vague empiric treatment guidelines coupled with increased time from specimen testing to getting test results and inadequate follow-up [66Feltes A, Combs J, Reynolds M, Conroy M, Lindsey S, Dick M, Li J, Reichert E. Impact of point-of-care gonorrhea and chlamydia testing in the emergency department on reducing overtreatment rates. Am J Emerg Med. 2024 Sep;83:64-68. doi: 10.1016/j.ajem.2024.06.040. Epub 2024 Jul 1. PMID: 38968852.]. With a turnaround time of at least 1 to 2 days, laboratory-confirmed results of traditional N gonorrhoeae and C trachomatis nucleic acid amplification tests are rarely available during a patient’s ED visit. Consequently, treatment decisions hinge on the emergency physician’s clinical judgement. Undertreatment of patients with a confirmed sexually transmitted infection increases the risk of transmission to subsequent sexual partners and potentially serious infectious complications. Overtreatment of women without a confirmed sexually transmitted infection results in excessive and inappropriate antibiotic use, a key driver of emerging antibiotic resistance [77Cherabie JN, Liang SY, Reno H. Diagnostics for Gonorrhea and Chlamydia in the Emergency Department: Fight Smarter Not Harder. Ann Emerg Med. 2021 Apr;77(4):411-413. doi: 10.1016/j.annemergmed.2020.09.445. PMID: 33766272.,88Gannon-Loew KE, Holland-Hall C. A review of current guidelines and research on the management of sexually transmitted infections in adolescents and young adults. Ther Adv Infect Dis. 2020 Oct 21;7:2049936120960664. doi: 10.1177/2049936120960664. PMID: 33598210; PMCID: PMC7863142.].
A Gram stain is a rapid and inexpensive test available in many Emergency Departments (EDs). It has historically been a critical tool in diagnosing STIs, particularly gonorrhea, as it allows for rapid identification of the causative bacteria, which appear as gram-negative diplococci under a microscope [33Schneider K, FitzGerald M, Byczkowski T, Reed J. Screening for Asymptomatic Gonorrhea and Chlamydia in the Pediatric Emergency Department. Sex Transm Dis. 2016 Apr;43(4):209-15. doi: 10.1097/OLQ.0000000000000424. PMID: 26967296.]. In women with positive cervical culture results, the Gram stain results from the endocervix are 50% - 60% sensitive and 82-97% specific. In addition, the presence of more than 10 PMNs per high-power field on an endocervical smear is consistent with cervicitis [99Qureshi S. Gonorrhea Workup July 2024. Medscape. https://emedicine.medscape.com/article/218059-workup.]. While Gram stain results alone are insufficient for the diagnosis of STIs in women, the results may be used in combination with clinical symptoms. In many EDs, the gram-stain evaluation of the endocervical flora may provide the only immediate laboratory evidence on which a clinical diagnosis can be based [1010Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021 Jul 23;70(4):1-187. doi: 10.15585/mmwr.rr7004a1. PMID: 34292926; PMCID: PMC8344968.]. For these reasons, a clear understanding of the diagnostic metrics of this test in a pragmatic setting is needed. Our aim was to evaluate the performance characteristics of endocervical Gram smears in the diagnosis of Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis in a female adolescent population presenting to the ED with genitourinary complaints.
We conducted a retrospective, cohort analysis of consecutive females (ages 13-19) with lower abdominal pain or genitourinary complaints seen at three academic medical centers over a two-year study period. These hospitals included Corewell Health Hospital-Butterworth Campus, Corewell Health Hospital-Blodgett campus, and DeVos Children’s Hospital. The combined annual ED census was approximately 190,000 during the study period. The common characteristic of these ED patients was that their chief complaint led the emergency physician to perform a pelvic exam with diagnostic testing for STI using endocervical/vaginal swabs. Positive criteria for a Gram stain included greater than 10 white blood cells per high-power field, gram-negative intracellular/extracellular diplococci (suggesting GC), or direct visualization of TV organisms. Quantitative Polymerase Chain Reaction (PCR) assays were used as the gold standard definition for CT/GC infection. The specimens were processed by using PCR amplification assays for both GC and CT (Abbott m2000, Des Plaines, IL). The turnaround time for study results was approximately 24 h among participating hospitals. Direct microscopic visualization of organisms on a separate wet mount prep was considered the reference standard for TV infection. Adolescents who had repeat visits to the ED for the same STI, which was initially untreated or undertreated, were excluded from the study. Additional exclusion criteria included patients with missing data, or those who presented after sexual assault since each hospital has different guidelines for empiric treatment for this subgroup of patients.
In patients with positive PCR assays for GC and/or CT, the ED physician or quality assurance coordinator confirmed by chart review whether the patient received appropriate antibiotic therapy according to standard CDC guidelines [1010Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021 Jul 23;70(4):1-187. doi: 10.15585/mmwr.rr7004a1. PMID: 34292926; PMCID: PMC8344968.]. The clinician-initiated telephone follow-up for antibiotic treatment in cases with positive results in which the patient was not treated at the time of the ED visit. Each participating hospital kept a log of the medical record including test results, how long it took to treat each positive patient, and a record of all patients who could not be treated. Successful follow-up was defined as contacting the patient and providing proper antibiotics. The number of attempts and the reasons for unsuccessful follow-up were also noted.
Standardized abstraction forms were used to obtain relevant patient information from ED medical records (Appendix). Patient demographics included age, race/ethnicity, insurance status, primary care physician, pregnancy, and risk factors for STI. Clinical features included signs, symptoms, duration, and pain intensity. Using a 0 to 10 numeric rating scale, the triage nurse asked patients to rate their pain intensity. Laboratory data provided urinary analysis, pregnancy tests, Gram stain results, wet mount, and PCR results for GC or CT. Treatment administered in the ED and prescriptions given to the patient on telephone follow-up were subsequently recorded.
All data were collected by four research associates who were blinded to the study objective. Research staff were trained in data abstraction using a set of mock case records. One researcher oversaw data collection and confirmed that variable definitions were uniformly applied. A second investigator performed a blinded critical review of a random sample of 10% of the programs to determine the reliability of data collection using kappa statistics. The primary outcome of this study was to evaluate the performance characteristics of endocervical Gram smears in the diagnosis of STI using sensitivity, specificity, and Likelihood Ratio (LR). We used 95% Confidence Intervals (CIs) for quantifying uncertainty. The PCR results were used as the gold standard to calculate sensitivity, specificity, and likelihood ratios of endocervical Gram stains for CT/GC infection and the wet mount was used as the reference standard for TV infection. We used 95% confidence intervals (CIs) for quantifying uncertainty. Secondary outcomes were the proportion of adolescent females being untreated in the participating EDs, the time to treatment, and the proportion lost to follow-up. Patients were considered lost to follow-up after three telephone attempts to establish communication and a written notice was sent to their provided address.
Data were entered into the Microsoft Excel database (Microsoft Corporation, Redmond, WA). Analyses were performed using SPSS statistical software (SPSS Inc., Chicago, IL). Descriptive statistics were used to describe demographic variables and clinical findings. Results were expressed as the mean ± SD. Discrete variables were analyzed by two-tailed unpaired t - tests, and Wilcoxon rank-sum and Chi-squared tests for continuous and ordinal data. This retrospective study was approved by the Corewell Health Institutional Review Board (# 2021-164).
During the study period, 1303 adolescent females were evaluated for genitourinary complaints. The mean age was 17.4 + 1.8 years. Common symptoms included abdominal/pelvic pain (53.0%), nausea/vomiting (44.4%), abnormal vaginal discharge (37.2%), urinary complaints (29.3%), and vaginal bleeding (6.6%). The average duration of symptoms prior to presentation was 5.3 + 6.0 days. A total of 318 adolescents (24.4%) had a positive pregnancy test documented in the ED.
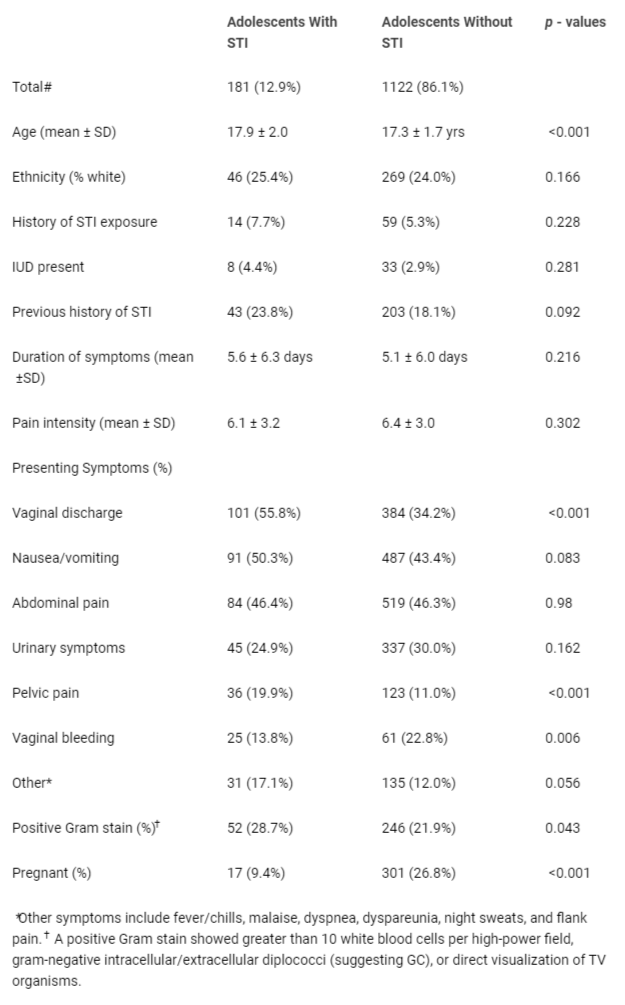
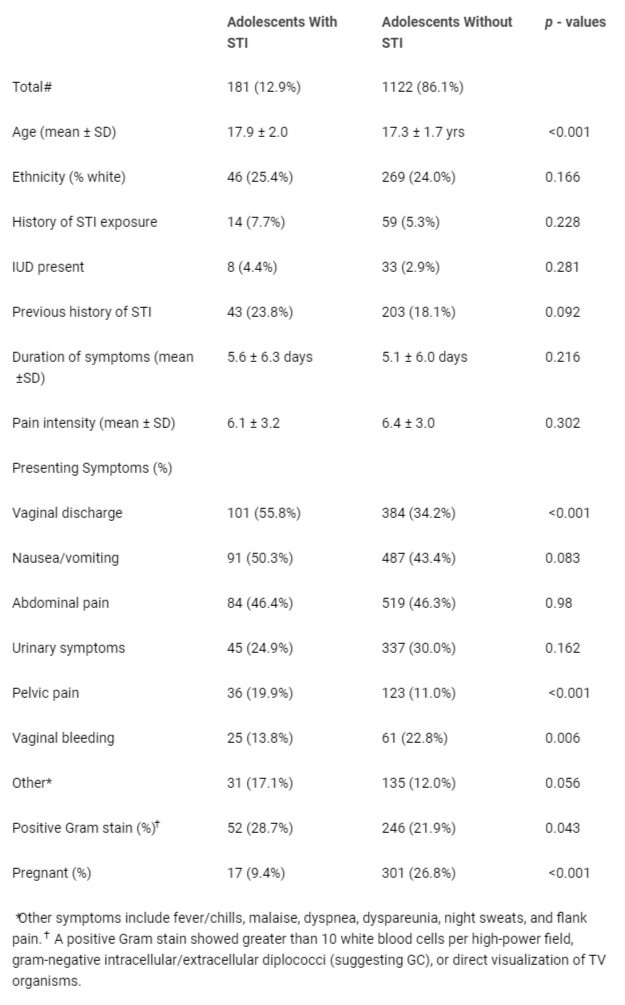
Overall, 181 adolescents (12.9%; 95% CI, 12.5 to 16.3%) had at least one documented STI while 24 patients (1.9%; 95% CI, 1.3 to 2.8%) had two or more infections. The most common STI diagnosis was Chlamydia trachomatis documented in 105 adolescents (8.1%). This was followed by Trichomonas vaginalis (4.6%) and Neisseria gonorrhoeae (3.2%). Table 1 compares the demographics and clinical findings in adolescents with and those without documented STI.
Table 1: Demographics and presenting complaints in adolescent women with and those without documented sexually transmitted infection (STI).
Patients with STIs tended to be younger, had complaints of vaginal discharge/bleeding, pelvic pain, and were more likely to have a positive Gram stain (28.7% vs. 21.9%).
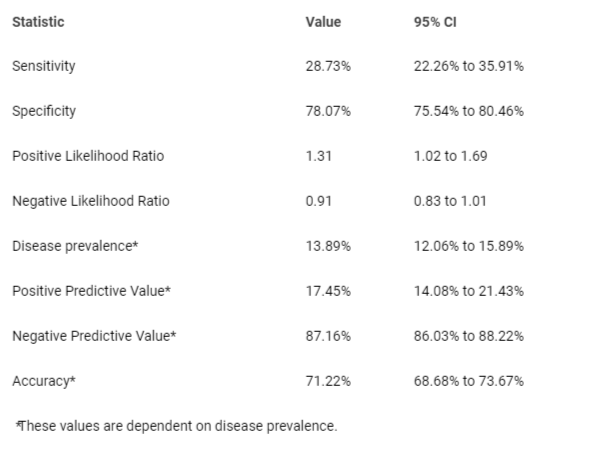
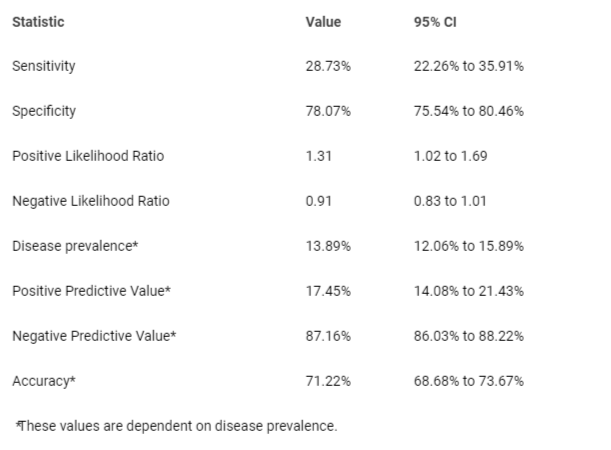
A total of 298 patients (22.9%) had a positive gram stain. The sensitivity, specificity, and positive likelihood ratio for Gram stain in the diagnosis of STI were 28.7% (95% CI, 22.2 to 35.9), 78.1% (95% CI, 75.5 to 80.5) and 1.31 (95% CI, 1.0 to 1.7), respectively (Table 2). The sensitivity of Gram stain to Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis were 35.9% (95% CI, 26.8 to 45.8), 34.5% (95% CI, 18.0 to 54.3), and 5.7% (95% CI, 1.3 to 15.7), respectively. Despite these poor diagnostic metrics, the 298 adolescents with a positive Gram stain were statistically more likely to receive antibiotics to empirically treat CT/GC infection (p = 0.041).
Table 2: Diagnostic indices for endocervical Gram smears in the diagnosis of STIs in a female adolescent population with genitourinary complaints.
Of the 1122 adolescents without a documented STI, 329 (29.3%) were treated empirically in the ED with antibiotics for presumed STI. In comparison, of the 145 adolescents who had positive PCR studies for Chlamydia trachomatis and/or Neisseria gonorrhoeae, 72 (49.7%) were not treated with antibiotics in the ED. Despite being combined with other clinical findings, the Gram stain likely contributed to the large numbers of adolescents overtreated (29.3%) or undertreated (49.7%) for CT/GC infection in the ED. Other factors such as age, insurance status, ethnic or cultural background, or known STI exposure were not associated with antibiotic treatment in the ED. Eighteen percent of the untreated STI patients had no complaints of pain or tenderness on pelvic examination. Untreated patients were more likely to have a discharge diagnosis of urinary tract infection (33.3%), vaginitis (30.6%), and first-trimester pregnancy (27.8%).
Of the 72 untreated patients with documented STI, 49 (68.1%) were subsequently contacted by phone and/or mail for antibiotics. The mean time interval between ED presentation and antibiotic treatment in these adolescents was 4.1 days (range, 1- 23 days). Overall, 23 (31.9%) of the untreated adolescents with STI were lost to follow-up. The consistency of data recording between investigators was excellent, with a median kappa statistic of 0.89.
Endocervical Gram stains taken during a pelvic examination are easy to perform and interpret. However, the positive likelihood ratio of inflammation on endocervical Gram stain (1.3 in adolescent women) is too low to recommend its use to direct empiric treatment in adolescents at risk for sexually transmitted infections. Diagnostic uncertainty or treatment failures should prompt specific laboratory testing. Our findings align with previously reported studies in adults that suggest that Gram stains should not be used alone as a diagnostic method for CT and NG [1111Berntsson M, Tunbäck P. Clinical and microscopic signs of cervicitis and urethritis: correlation with Chlamydia trachomatis infection in female STI patients. Acta Derm Venereol. 2013 Mar 27;93(2):230-3. doi: 10.2340/00015555-1536. PMID: 23460336.-1414Myziuk L, Romanowski B, Brown M. Endocervical Gram stain smears and their usefulness in the diagnosis of Chlamydia trachomatis. Sex Transm Infect. 2001 Apr;77(2):103-6. doi: 10.1136/sti.77.2.103. PMID: 11287687; PMCID: PMC1744259.].However, this test continues to be used in many settings, including those that provide dedicated STI testing [33Schneider K, FitzGerald M, Byczkowski T, Reed J. Screening for Asymptomatic Gonorrhea and Chlamydia in the Pediatric Emergency Department. Sex Transm Dis. 2016 Apr;43(4):209-15. doi: 10.1097/OLQ.0000000000000424. PMID: 26967296.,44Breslin K, Tuchman L, Hayes KL, Badolato G, Goyal MK. Sensitivity and Specificity of Empiric Treatment for Sexually Transmitted Infections in a Pediatric Emergency Department. J Pediatr. 2017 Oct;189:48-53. doi: 10.1016/j.jpeds.2017.05.050. Epub 2017 Jun 17. PMID: 28629687; PMCID: PMC5614813.,1515Rompalo AM, Castleberry N, Widdice L, Schulkin J, Gaydos CA. Patterns of point-of-care test use among obstetricians and gynaecologists in the US. Sex Health. 2018 Jul;15(4):318-324. doi: 10.1071/SH17180. PMID: 29914611; PMCID: PMC6450764.].The children’s hospital affiliated with this study performs over 3000 endocervical gram stains each year.
Adolescent patients with STIs often present to the ED with vague symptoms that lead to an unclear diagnosis [33Schneider K, FitzGerald M, Byczkowski T, Reed J. Screening for Asymptomatic Gonorrhea and Chlamydia in the Pediatric Emergency Department. Sex Transm Dis. 2016 Apr;43(4):209-15. doi: 10.1097/OLQ.0000000000000424. PMID: 26967296.,44Breslin K, Tuchman L, Hayes KL, Badolato G, Goyal MK. Sensitivity and Specificity of Empiric Treatment for Sexually Transmitted Infections in a Pediatric Emergency Department. J Pediatr. 2017 Oct;189:48-53. doi: 10.1016/j.jpeds.2017.05.050. Epub 2017 Jun 17. PMID: 28629687; PMCID: PMC5614813.]. PCR assays for GC and CT may return several days after the initial visit, and studies have shown significant loss-to-follow-up rates for untreated adolescents [1616Uppal A, Chou KJ. Screening adolescents for sexually transmitted infections in the pediatric emergency department. Pediatr Emerg Care. 2015 Jan;31(1):20-4. doi: 10.1097/PEC.0000000000000322. PMID: 25526018.,1717Pattishall AE, Rahman SY, Jain S, Simon HK. Empiric treatment of sexually transmitted infections in a pediatric Emergency Department: are we making the right decisions? Am J Emerg Med. 2012 Oct;30(8):1588-90. doi: 10.1016/j.ajem.2011.09.028. Epub 2011 Dec 12. PMID: 22169584.]. A previous study at our institution showed that approximately 70% of adolescents aged 13–19 years with a positive PCR test result for GC or CT were not initially treated in the ED [1818Krivochenitser R, Bicker E, Whalen D, Gardiner C, Jones JS. Adolescent women with sexually transmitted infections: who gets lost to follow-up? J Emerg Med. 2014 Nov;47(5):507-12. doi: 10.1016/j.jemermed.2014.06.022. Epub 2014 Aug 22. PMID: 25154560.]. Furthermore, over 40% of those patients discharged from the ED without treatment were unable to be reached by telephone or mail, and thus were ‘‘lost to follow-up’’ [1818Krivochenitser R, Bicker E, Whalen D, Gardiner C, Jones JS. Adolescent women with sexually transmitted infections: who gets lost to follow-up? J Emerg Med. 2014 Nov;47(5):507-12. doi: 10.1016/j.jemermed.2014.06.022. Epub 2014 Aug 22. PMID: 25154560.]. Due to these difficulties, emergency physicians may choose to empirically treat for STI when they have a positive endocervical gram stain.
Gram stain is a rapid and inexpensive test available in many emergency departments [99Qureshi S. Gonorrhea Workup July 2024. Medscape. https://emedicine.medscape.com/article/218059-workup.]. This is very useful if the clinician has easy access to a microscope because the diagnosis may be made without waiting for PCR results. An excess of leukocytes (more than 10 PMNs per high-power field) in the endocervical mucous is consistent with chlamydial and gonococcal cervicitis [1212Stefanski P, Hafner JW, Riley SL, Sunga KL, Schaefer TJ. Diagnostic utility of the genital Gram stain in ED patients. Am J Emerg Med. 2010 Jan;28(1):13-8. doi: 10.1016/j.ajem.2008.09.016. PMID: 20006195.]. In women who lack a cervix because of hysterectomy, a urethral culture is used to make the diagnosis [99Qureshi S. Gonorrhea Workup July 2024. Medscape. https://emedicine.medscape.com/article/218059-workup.]. Unfortunately, the results of this current study show the sensitivity of gram stain results to be 29% sensitive and 78% specific for cervicitis in women.
Several factors can complicate the diagnosis and empiric treatment of STIs, including pregnancy, atypical presentation, concurrent urine infection, vaginal bleeding, vulvovaginitis, and the age of the patient [1010Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021 Jul 23;70(4):1-187. doi: 10.15585/mmwr.rr7004a1. PMID: 34292926; PMCID: PMC8344968.]. Pregnant patients with GC or CT are rarely treated in the ED upon presentation due to a lack of rapid testing and nonspecific complaints [1818Krivochenitser R, Bicker E, Whalen D, Gardiner C, Jones JS. Adolescent women with sexually transmitted infections: who gets lost to follow-up? J Emerg Med. 2014 Nov;47(5):507-12. doi: 10.1016/j.jemermed.2014.06.022. Epub 2014 Aug 22. PMID: 25154560.,1919Ouellette L, Wigstadt S, Nicholson A, Zamarripa A, Jones J. Emergency department utilization by newly pregnant adolescents: A community-based study. Am J Emerg Med. 2019 Feb;37(2):358-360. doi: 10.1016/j.ajem.2018.06.028. Epub 2018 Jun 13. PMID: 29929889.]. Perhaps the main reason for the lack of antibiotic treatment in this specific population is the young age of the patient. However, the age at which young people begin having sexual intercourse has markedly decreased in the United States, and clinicians should consider cervicitis in their differential diagnosis when treating patients even as young as 13 years of age [1616Uppal A, Chou KJ. Screening adolescents for sexually transmitted infections in the pediatric emergency department. Pediatr Emerg Care. 2015 Jan;31(1):20-4. doi: 10.1097/PEC.0000000000000322. PMID: 25526018.-1818Krivochenitser R, Bicker E, Whalen D, Gardiner C, Jones JS. Adolescent women with sexually transmitted infections: who gets lost to follow-up? J Emerg Med. 2014 Nov;47(5):507-12. doi: 10.1016/j.jemermed.2014.06.022. Epub 2014 Aug 22. PMID: 25154560.]. Furthermore, there are ethical-legal questions regarding reporting to proper authorities when STIs are diagnosed in this underage population.
Screening and treating adolescent ED patients for STIs is paramount. If left untreated, STIs may result in further complications, including acute pelvic inflammatory disease, ectopic pregnancy, and infertility [1818Krivochenitser R, Bicker E, Whalen D, Gardiner C, Jones JS. Adolescent women with sexually transmitted infections: who gets lost to follow-up? J Emerg Med. 2014 Nov;47(5):507-12. doi: 10.1016/j.jemermed.2014.06.022. Epub 2014 Aug 22. PMID: 25154560.]. Culturing organisms takes several days and requires close patient follow-up. Rapid point-of-care testing methods, such as DNA probes, have high sensitivity and specificity [99Qureshi S. Gonorrhea Workup July 2024. Medscape. https://emedicine.medscape.com/article/218059-workup.,1515Rompalo AM, Castleberry N, Widdice L, Schulkin J, Gaydos CA. Patterns of point-of-care test use among obstetricians and gynaecologists in the US. Sex Health. 2018 Jul;15(4):318-324. doi: 10.1071/SH17180. PMID: 29914611; PMCID: PMC6450764.]. Ideally, STI testing should be completed in a timely manner, produce accurate results, and be priced affordably [2020Kazmir S, Pierce MC, Simonton K, Rodean J, Neuman MI, Simon NE, Alpern ER. Pediatric Emergency Department Testing for Gonorrhea and Chlamydia in Children. Pediatr Emerg Care. 2022 Jun 1;38(6):247-252. doi: 10.1097/PEC.0000000000002637. Epub 2022 Feb 21. PMID: 35639429.]. Only then can we expect the rates of pelvic inflammatory disease and other STI morbidities to be reduced in our adolescent population.
Several limitations were present in our study. Given that this was a retrospective review of medical charts, there is inherent variability in the assessment and documentation of clinical information by different providers. Therefore, documentation of outcome variables of interest may not have been consistent. Another limitation is that some of the patient population findings in our cohort may be more specific to our region and local culture, which may not translate to every adolescent population. Finally, the small number of adolescents with STIs in our population limited the precision of our findings and resulted in wider confidence intervals.
Sexually transmitted infections in adolescents are a significant public health burden that can lead to severe morbidity if left untreated. Emergency departments are often the first and only point of contact for these patients in the healthcare setting. The positive likelihood ratio of inflammation on endocervical Gram stain is too low to recommend its use to direct empiric treatment in adolescents at risk for sexually transmitted infections. Further research should include liberal policies to treat less symptomatic patients empirically, accentuate point-of-contact testing, and better mechanisms for contact and follow-up after hospital or clinic discharge.
Vayngortin T, Gracia M, Clark K, Vayngortin B, Bialostozky M, Heitzman L, Hollenbach K, Kumar M, Titchen K, Bryl A. Increasing Chlamydia and Gonorrhea Testing for Adolescents in the Pediatric Emergency Department. Pediatrics. 2024 Jan 1;153(1):e2022059707. doi: 10.1542/peds.2022-059707. PMID: 38053440; PMCID: PMC11022968.
Shannon CL, Klausner JD. The growing epidemic of sexually transmitted infections in adolescents: a neglected population. Curr Opin Pediatr. 2018 Feb;30(1):137-143. doi: 10.1097/MOP.0000000000000578. PMID: 29315111; PMCID: PMC5856484.
Schneider K, FitzGerald M, Byczkowski T, Reed J. Screening for Asymptomatic Gonorrhea and Chlamydia in the Pediatric Emergency Department. Sex Transm Dis. 2016 Apr;43(4):209-15. doi: 10.1097/OLQ.0000000000000424. PMID: 26967296.
Breslin K, Tuchman L, Hayes KL, Badolato G, Goyal MK. Sensitivity and Specificity of Empiric Treatment for Sexually Transmitted Infections in a Pediatric Emergency Department. J Pediatr. 2017 Oct;189:48-53. doi: 10.1016/j.jpeds.2017.05.050. Epub 2017 Jun 17. PMID: 28629687; PMCID: PMC5614813.
Anaene M, Soyemi K, Caskey R. Factors associated with the over-treatment and under-treatment of gonorrhea and chlamydia in adolescents presenting to a public hospital emergency department. Int J Infect Dis. 2016 Dec;53:34-38. doi: 10.1016/j.ijid.2016.10.009. Epub 2016 Oct 19. PMID: 27771470.
Feltes A, Combs J, Reynolds M, Conroy M, Lindsey S, Dick M, Li J, Reichert E. Impact of point-of-care gonorrhea and chlamydia testing in the emergency department on reducing overtreatment rates. Am J Emerg Med. 2024 Sep;83:64-68. doi: 10.1016/j.ajem.2024.06.040. Epub 2024 Jul 1. PMID: 38968852.
Cherabie JN, Liang SY, Reno H. Diagnostics for Gonorrhea and Chlamydia in the Emergency Department: Fight Smarter Not Harder. Ann Emerg Med. 2021 Apr;77(4):411-413. doi: 10.1016/j.annemergmed.2020.09.445. PMID: 33766272.
Gannon-Loew KE, Holland-Hall C. A review of current guidelines and research on the management of sexually transmitted infections in adolescents and young adults. Ther Adv Infect Dis. 2020 Oct 21;7:2049936120960664. doi: 10.1177/2049936120960664. PMID: 33598210; PMCID: PMC7863142.
Qureshi S. Gonorrhea Workup July 2024. Medscape. https://emedicine.medscape.com/article/218059-workup.
Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021 Jul 23;70(4):1-187. doi: 10.15585/mmwr.rr7004a1. PMID: 34292926; PMCID: PMC8344968.
Berntsson M, Tunbäck P. Clinical and microscopic signs of cervicitis and urethritis: correlation with Chlamydia trachomatis infection in female STI patients. Acta Derm Venereol. 2013 Mar 27;93(2):230-3. doi: 10.2340/00015555-1536. PMID: 23460336.
Stefanski P, Hafner JW, Riley SL, Sunga KL, Schaefer TJ. Diagnostic utility of the genital Gram stain in ED patients. Am J Emerg Med. 2010 Jan;28(1):13-8. doi: 10.1016/j.ajem.2008.09.016. PMID: 20006195.
Hobbs MM, Seña AC. Modern diagnosis of Trichomonas vaginalis infection. Sex Transm Infect. 2013 Sep;89(6):434-8. doi: 10.1136/sextrans-2013-051057. Epub 2013 Apr 30. PMID: 23633669; PMCID: PMC3787709.
Myziuk L, Romanowski B, Brown M. Endocervical Gram stain smears and their usefulness in the diagnosis of Chlamydia trachomatis. Sex Transm Infect. 2001 Apr;77(2):103-6. doi: 10.1136/sti.77.2.103. PMID: 11287687; PMCID: PMC1744259.
Rompalo AM, Castleberry N, Widdice L, Schulkin J, Gaydos CA. Patterns of point-of-care test use among obstetricians and gynaecologists in the US. Sex Health. 2018 Jul;15(4):318-324. doi: 10.1071/SH17180. PMID: 29914611; PMCID: PMC6450764.
Uppal A, Chou KJ. Screening adolescents for sexually transmitted infections in the pediatric emergency department. Pediatr Emerg Care. 2015 Jan;31(1):20-4. doi: 10.1097/PEC.0000000000000322. PMID: 25526018.
Pattishall AE, Rahman SY, Jain S, Simon HK. Empiric treatment of sexually transmitted infections in a pediatric Emergency Department: are we making the right decisions? Am J Emerg Med. 2012 Oct;30(8):1588-90. doi: 10.1016/j.ajem.2011.09.028. Epub 2011 Dec 12. PMID: 22169584.
Krivochenitser R, Bicker E, Whalen D, Gardiner C, Jones JS. Adolescent women with sexually transmitted infections: who gets lost to follow-up? J Emerg Med. 2014 Nov;47(5):507-12. doi: 10.1016/j.jemermed.2014.06.022. Epub 2014 Aug 22. PMID: 25154560.
Ouellette L, Wigstadt S, Nicholson A, Zamarripa A, Jones J. Emergency department utilization by newly pregnant adolescents: A community-based study. Am J Emerg Med. 2019 Feb;37(2):358-360. doi: 10.1016/j.ajem.2018.06.028. Epub 2018 Jun 13. PMID: 29929889.
Kazmir S, Pierce MC, Simonton K, Rodean J, Neuman MI, Simon NE, Alpern ER. Pediatric Emergency Department Testing for Gonorrhea and Chlamydia in Children. Pediatr Emerg Care. 2022 Jun 1;38(6):247-252. doi: 10.1097/PEC.0000000000002637. Epub 2022 Feb 21. PMID: 35639429.
Nanda S, Schoonover A, Kaur J, Vu A, Tavares E, Zamarripa A, Kolacki C, Ouellette L, Jones J. Screening for Sexually Transmitted Infections in Adolescents with Genitourinary Complaints: Is There a Still Role for Endocervical Gram Stains?. IgMin Res. . October 16, 2024; 2(10): 807-811. IgMin ID: igmin251; DOI:10.61927/igmin251; Available at: igmin.link/p251
1College of Human Medicine, Michigan State University, Grand Rapids, MI, USA
2Corewell Health Department of Emergency Medicine, Grand Rapids, MI, USA
3Helen DeVos Children’s Hospital, Grand Rapids, MI, USA
Address Correspondence: Jeffrey Jones, Corewell Health Department of Emergency Medicine, Grand Rapids, USA, Email: [email protected]; [email protected]
How to cite this article: Nanda S, Schoonover A, Kaur J, Vu A, Tavares E, Zamarripa A, Kolacki C, Ouellette L, Jones J. Screening for Sexually Transmitted Infections in Adolescents with Genitourinary Complaints: Is There a Still Role for Endocervical Gram Stains?. IgMin Res. . October 16, 2024; 2(10): 807-811. IgMin ID: igmin251; DOI:10.61927/igmin251; Available at: igmin.link/p251
Table 1: Demographics and presenting complaints in adolesce...
Table 2: Diagnostic indices for endocervical Gram smears in...
Vayngortin T, Gracia M, Clark K, Vayngortin B, Bialostozky M, Heitzman L, Hollenbach K, Kumar M, Titchen K, Bryl A. Increasing Chlamydia and Gonorrhea Testing for Adolescents in the Pediatric Emergency Department. Pediatrics. 2024 Jan 1;153(1):e2022059707. doi: 10.1542/peds.2022-059707. PMID: 38053440; PMCID: PMC11022968.
Shannon CL, Klausner JD. The growing epidemic of sexually transmitted infections in adolescents: a neglected population. Curr Opin Pediatr. 2018 Feb;30(1):137-143. doi: 10.1097/MOP.0000000000000578. PMID: 29315111; PMCID: PMC5856484.
Schneider K, FitzGerald M, Byczkowski T, Reed J. Screening for Asymptomatic Gonorrhea and Chlamydia in the Pediatric Emergency Department. Sex Transm Dis. 2016 Apr;43(4):209-15. doi: 10.1097/OLQ.0000000000000424. PMID: 26967296.
Breslin K, Tuchman L, Hayes KL, Badolato G, Goyal MK. Sensitivity and Specificity of Empiric Treatment for Sexually Transmitted Infections in a Pediatric Emergency Department. J Pediatr. 2017 Oct;189:48-53. doi: 10.1016/j.jpeds.2017.05.050. Epub 2017 Jun 17. PMID: 28629687; PMCID: PMC5614813.
Anaene M, Soyemi K, Caskey R. Factors associated with the over-treatment and under-treatment of gonorrhea and chlamydia in adolescents presenting to a public hospital emergency department. Int J Infect Dis. 2016 Dec;53:34-38. doi: 10.1016/j.ijid.2016.10.009. Epub 2016 Oct 19. PMID: 27771470.
Feltes A, Combs J, Reynolds M, Conroy M, Lindsey S, Dick M, Li J, Reichert E. Impact of point-of-care gonorrhea and chlamydia testing in the emergency department on reducing overtreatment rates. Am J Emerg Med. 2024 Sep;83:64-68. doi: 10.1016/j.ajem.2024.06.040. Epub 2024 Jul 1. PMID: 38968852.
Cherabie JN, Liang SY, Reno H. Diagnostics for Gonorrhea and Chlamydia in the Emergency Department: Fight Smarter Not Harder. Ann Emerg Med. 2021 Apr;77(4):411-413. doi: 10.1016/j.annemergmed.2020.09.445. PMID: 33766272.
Gannon-Loew KE, Holland-Hall C. A review of current guidelines and research on the management of sexually transmitted infections in adolescents and young adults. Ther Adv Infect Dis. 2020 Oct 21;7:2049936120960664. doi: 10.1177/2049936120960664. PMID: 33598210; PMCID: PMC7863142.
Qureshi S. Gonorrhea Workup July 2024. Medscape. https://emedicine.medscape.com/article/218059-workup.
Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021 Jul 23;70(4):1-187. doi: 10.15585/mmwr.rr7004a1. PMID: 34292926; PMCID: PMC8344968.
Berntsson M, Tunbäck P. Clinical and microscopic signs of cervicitis and urethritis: correlation with Chlamydia trachomatis infection in female STI patients. Acta Derm Venereol. 2013 Mar 27;93(2):230-3. doi: 10.2340/00015555-1536. PMID: 23460336.
Stefanski P, Hafner JW, Riley SL, Sunga KL, Schaefer TJ. Diagnostic utility of the genital Gram stain in ED patients. Am J Emerg Med. 2010 Jan;28(1):13-8. doi: 10.1016/j.ajem.2008.09.016. PMID: 20006195.
Hobbs MM, Seña AC. Modern diagnosis of Trichomonas vaginalis infection. Sex Transm Infect. 2013 Sep;89(6):434-8. doi: 10.1136/sextrans-2013-051057. Epub 2013 Apr 30. PMID: 23633669; PMCID: PMC3787709.
Myziuk L, Romanowski B, Brown M. Endocervical Gram stain smears and their usefulness in the diagnosis of Chlamydia trachomatis. Sex Transm Infect. 2001 Apr;77(2):103-6. doi: 10.1136/sti.77.2.103. PMID: 11287687; PMCID: PMC1744259.
Rompalo AM, Castleberry N, Widdice L, Schulkin J, Gaydos CA. Patterns of point-of-care test use among obstetricians and gynaecologists in the US. Sex Health. 2018 Jul;15(4):318-324. doi: 10.1071/SH17180. PMID: 29914611; PMCID: PMC6450764.
Uppal A, Chou KJ. Screening adolescents for sexually transmitted infections in the pediatric emergency department. Pediatr Emerg Care. 2015 Jan;31(1):20-4. doi: 10.1097/PEC.0000000000000322. PMID: 25526018.
Pattishall AE, Rahman SY, Jain S, Simon HK. Empiric treatment of sexually transmitted infections in a pediatric Emergency Department: are we making the right decisions? Am J Emerg Med. 2012 Oct;30(8):1588-90. doi: 10.1016/j.ajem.2011.09.028. Epub 2011 Dec 12. PMID: 22169584.
Krivochenitser R, Bicker E, Whalen D, Gardiner C, Jones JS. Adolescent women with sexually transmitted infections: who gets lost to follow-up? J Emerg Med. 2014 Nov;47(5):507-12. doi: 10.1016/j.jemermed.2014.06.022. Epub 2014 Aug 22. PMID: 25154560.
Ouellette L, Wigstadt S, Nicholson A, Zamarripa A, Jones J. Emergency department utilization by newly pregnant adolescents: A community-based study. Am J Emerg Med. 2019 Feb;37(2):358-360. doi: 10.1016/j.ajem.2018.06.028. Epub 2018 Jun 13. PMID: 29929889.
Kazmir S, Pierce MC, Simonton K, Rodean J, Neuman MI, Simon NE, Alpern ER. Pediatric Emergency Department Testing for Gonorrhea and Chlamydia in Children. Pediatr Emerg Care. 2022 Jun 1;38(6):247-252. doi: 10.1097/PEC.0000000000002637. Epub 2022 Feb 21. PMID: 35639429.