Welcome to IgMin Research – an Open Access journal uniting Biology, Medicine, and Engineering. We’re dedicated to advancing global knowledge and fostering collaboration across scientific fields.
Welcome to IgMin, a leading platform dedicated to enhancing knowledge dissemination and professional growth across multiple fields of science, technology, and the humanities. We believe in the power of open access, collaboration, and innovation. Our goal is to provide individuals and organizations with the tools they need to succeed in the global knowledge economy.
IgMin Publications Inc., Suite 102, West Hartford, CT - 06110, USA
The Model for Clinical, Laboratory, and Genetic Prediction of Recurrent Ischemic Stroke against the Background of Laboratory Aspirin Resistance using Machine Learning
The aim of the study was to determine the incidence of laboratory aspirin resistance; and to study the associations of genetic markers and clinical and laboratory parameters (including parameters of the platelet hemostasis) in patients with non-cardioembolic ischemic stroke using machine learning methods to assess the prognosis of recurrent ischemic strokes. Clinical and laboratory data (including induced platelet aggregation) were analyzed from 296 patients with ischemic stroke who were treated in the stroke center of City Clinical Hospital No. 1 named after. N.I. Pirogov. The frequencies of polymorphic variants of the ITGB3, GPIba, TBXA2R, ITGA2, PLA2G7, HMOX1, PTGS1, PTGS2, ADRA2A, ABCB1, PEAR1 genes and intergenic region 9p21.3) in patients with non-cardioembolic ischemic stroke, which were identified using hydrogel biochip technology, were determined. Using the developed machine learning model, additional clinical and genetic factors influencing the development of laboratory aspirin resistance and recurrent ischemic stroke were studied. In the future, the identified factors can be used for differentiated prevention of recurrent ischemic strokes.
This scientific work is part of a program to study the relationship of gene polymorphisms with clinical and laboratory data in patients with ischemic stroke [11Anisimova AV, Gunchenko AS, Ikonnikova AY, Galkin SS, Avdonina MA, Nasedkina TV. Kliniko-geneticheskiĭ analiz faktorov riska razvitiia ostroĭ i khronicheskoĭ ishemii golovnogo mozga [A clinical and genetic analysis of risk factors for the development of acute and chronic cerebral ischemia]. Zh Nevrol Psikhiatr Im S S Korsakova. 2019;119(3. Vyp. 2):62-67. Russian. doi: 10.17116/jnevro201911903262. PMID: 31184626.-55Storozhakov GI, Gendlin GE, Anisimova AV, Melekhov AV, Ostrovskaya YI. Taktika antigipertenzivnoĭ terapii u patsientov s gipertonicheskim krizom, oslozhnennym gemorragicheskim insul'tom [Tactics of antihypertensive therapy in patients with hypertonic crisis complicated with hemorrhagic stroke]. Zh Nevrol Psikhiatr Im S S Korsakova. 2015;115(3 Pt 2):12-19. Russian. doi: 10.17116/jnevro2015115312-19. PMID: 26120992.].
The frequency of development of ischemic non-cardioembolic (atherothrombotic and unspecified pathogenetic variants according to TOAST criteria) [66Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993 Jan;24(1):35-41. doi: 10.1161/01.str.24.1.35. PMID: 7678184.]) stroke remains consistently high both in Russia and around the world, despite the widespread functioning of a network of regional vascular centers and the introduction of innovative treatment methods such as thromboextraction [77Saini V, Guada L, Yavagal DR. Global Epidemiology of Stroke and Access to Acute Ischemic Stroke Interventions. Neurology. 2021 Nov 16;97(20 Suppl 2):S6-S16. doi: 10.1212/WNL.0000000000012781. PMID: 34785599.-1010Pohl M, Hesszenberger D, Kapus K, Meszaros J, Feher A, Varadi I, Pusch G, Fejes E, Tibold A, Feher G. Ischemic stroke mimics: A comprehensive review. J Clin Neurosci. 2021 Nov;93:174-182. doi: 10.1016/j.jocn.2021.09.025. Epub 2021 Sep 20. PMID: 34656244.]. The percentage of recurrent strokes is increasing and depends on many factors, such as the patient’s age, concomitant diseases, compliance, and many other circumstances. A variety of data on the incidence of recurrent strokes can be found in the literature.
According to many authors [1111Zheng S, Yao B. Impact of risk factors for recurrence after the first ischemic stroke in adults: A systematic review and meta-analysis. J Clin Neurosci. 2019 Feb;60:24-30. doi: 10.1016/j.jocn.2018.10.026. Epub 2018 Oct 16. PMID: 30340974.-1414Ding L, Liu Y, Meng X, Jiang Y, Lin J, Cheng S, Xu Z, Zhao X, Li H, Wang Y, Li Z. Biomarker and genomic analyses reveal molecular signatures of non-cardioembolic ischemic stroke. Signal Transduct Target Ther. 2023 May 30;8(1):222. doi: 10.1038/s41392-023-01465-w. PMID: 37248226; PMCID: PMC10227023.], genetic predisposition (increased risks of recurrent ischemic strokes have been identified in patients carrying certain gene polymorphisms) may also play a role in increasing the risk of recurrent ischemic stroke, since certain hereditary factors may contribute to a higher susceptibility to blood clots or atherosclerosis. Thus, the genes ITGB3, GPIba, TBXA2R, ITGA2, PLA2G7, HMOX1, PTGS1, PTGS2, ADRA2A, ABCB1, PEAR1 may influence susceptibility to ischemic stroke; platelet aggregation may be associated with the development of blood clots in blood vessels, as well as aspirin resistance [1515Dash P, Singh VK, Gautam D, Pathak A, Kumar A, Mishra SP, Dash D, Mishra VN, Joshi D, Chaurasia RN. Aspirin resistance and blood biomarkers in predicting ischemic stroke recurrence: An exploratory study. Brain Circ. 2022 Mar 21;8(1):31-37. doi: 10.4103/bc.bc_75_21. PMID: 35372727; PMCID: PMC8973447.-2424Silva GFD, Lopes BM, Moser V, Ferreira LE. Impact of pharmacogenetics on aspirin resistance: a systematic review. Arq Neuropsiquiatr. 2023 Jan;81(1):62-73. doi: 10.1055/s-0042-1758445. Epub 2023 Mar 14. PMID: 36918009; PMCID: PMC10014202.] which may be associated with disturbances in the biological processes involved in platelet aggregation.
Changes in platelet aggregation properties can occur in many pathological conditions, which can play a leading role, in addition to genetic factors, in the development of repeated ischemic strokes. Some studies suggest that approximately 25% - 30% of patients will have a second stroke within five years of the first event, but this percentage may also depend on the study population and data collection methods used. Obviously, the problem of preventing both primary and recurrent ischemic strokes remains relevant.
Laboratory resistance to aspirin refers to cases when patients do not experience suppression of platelet aggregation function during antiplatelet therapy with acetylsalicylic acid. This may be due to both genetic factors and other biological processes affecting platelet aggregation. Currently, the question of the role of individual genetic factors in the development of aspirin resistance has not been resolved.
Literary data indicate a fairly large percentage of recurrent ischemic strokes while taking both antiplatelet and anticoagulant therapy. Acetylsalicylic acid belongs to a group of drugs that act on the metabolism of arachidonic acid by inhibiting cyclooxygenase, which leads to the suppression of thromboxane A2 by platelets and reduces their aggregation.
Thus, given the variety of reasons that can lead to recurrent ischemic stroke, the high frequency of recurrent ischemic strokes indicates the need to develop individual programs taking into account risk factors. The development of modern computer technologies, including artificial intelligence and machine learning methods, can help solve this problem.
The aim of the study was to determine the incidence of laboratory aspirin resistance; to study the associations of genetic markers and clinical and laboratory parameters (including parameters of the platelet hemostasis) in patients with non-cardioembolic ischemic stroke using machine learning methods to assess the prognosis of recurrent ischemic strokes.
The study was conducted on the basis of the stroke center of City Clinical Hospital No. 1 named after. N.I. Pirogov from 2022 to 2023 Inclusion criteria were: 1) verified ischemic stroke; 2) Age from 45 years; 3) Non-cardioembolic pathogenetic variant of ischemic stroke according to TOAST criteria; 4) Opportunity to take part in the study. Exclusion criteria were: 1) neuroimaging signs of a brain tumor, arteriovenous malformation, brain abscess, vascular aneurysm; 2) surgery on the brain or spinal cord; 3) previous stroke or severe traumatic brain injury within 3 months; 4) severe liver diseases; 5) neoplasms with an increased risk of bleeding; 6) Cardioembolic pathogenetic variant of ischemic stroke; 7) operations or invasive procedures in the last 10 days; 8) data on bleeding or acute injury at the time of examination. The study was approved by the ethics committee of the Russian National Research Medical University named after. N.I. Pirogov No. 1567 dated February 10, 2022
The data of 296 patients with ischemic stroke were analyzed while they were in the stroke center of City Clinical Hospital No. 1 named after. N.I. Pirogov. All patients received therapy according to clinical guidelines for the treatment of ischemic stroke, including antiplatelet therapy (acetylsalicylic acid at a dose of 125 mg).
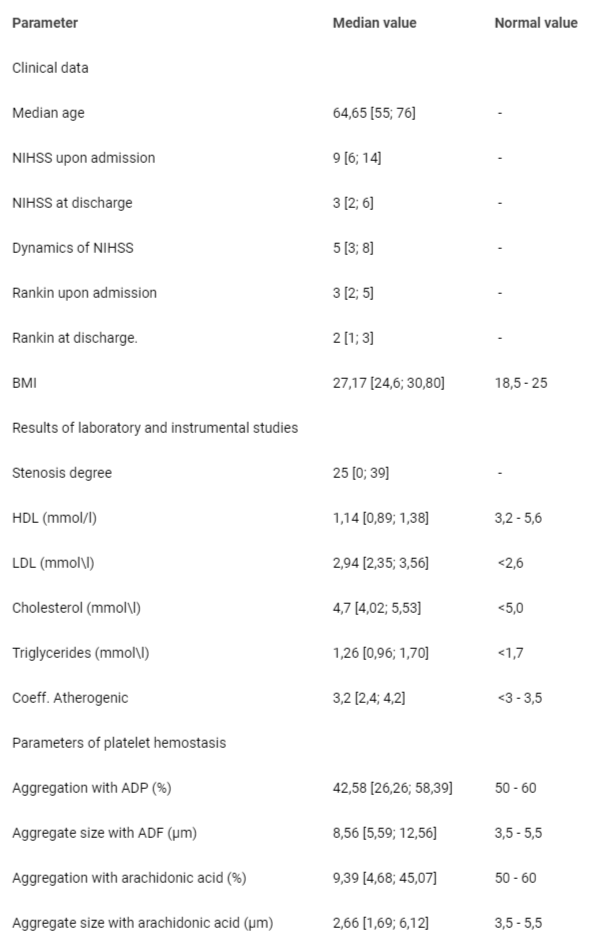
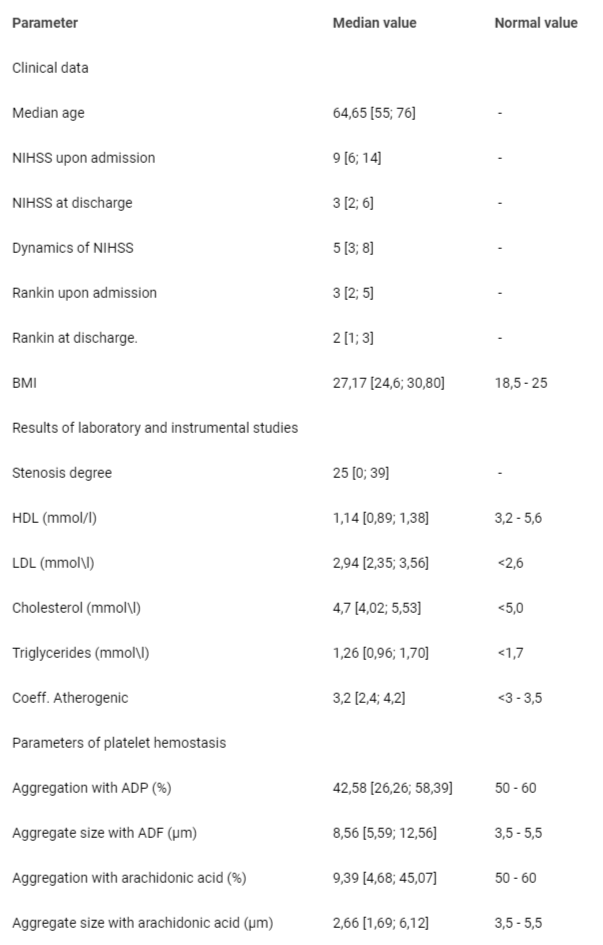
The average age of patients included in the study was 64.65 [55; 76] years. The median NIHSS score at admission was 9 [6; 146; 14Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993 Jan;24(1):35-41. doi: 10.1161/01.str.24.1.35. PMID: 7678184.], at the time of discharge 3 [2; 62; 6Anisimova AV, Gunchenko AS, Avdonina MA, Ikonnikova AU, Nasedkina TV. Clinical features and genetic risk factors in the development of ischemic stroke. Ural Medical Journal. 2017; T. 153: 9.], dynamics indicator 5 [3; 83; 8Anisimova AV, Gendlin GE, Borisov SN. [Prevention of stroke in patients with atrial fibrillation: a role of modern anticoagulants]. Zh Nevrol Psikhiatr Im S S Korsakova. 2013;113(9 Pt 2):62-9. Russian. PMID: 24107898.]. The main clinical and laboratory parameters (at admission) are presented in Table 1.
Table 1: Median values of the main clinical and laboratory parameters of patients with non-cardioembolic ischemic stroke.
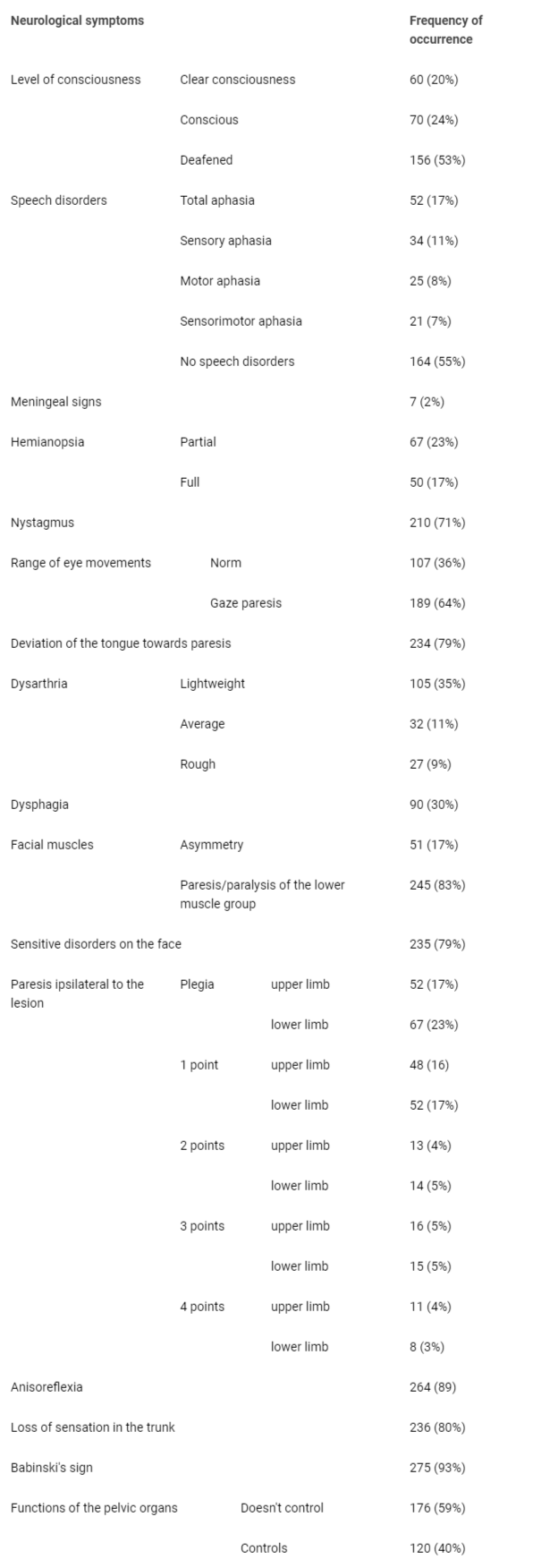
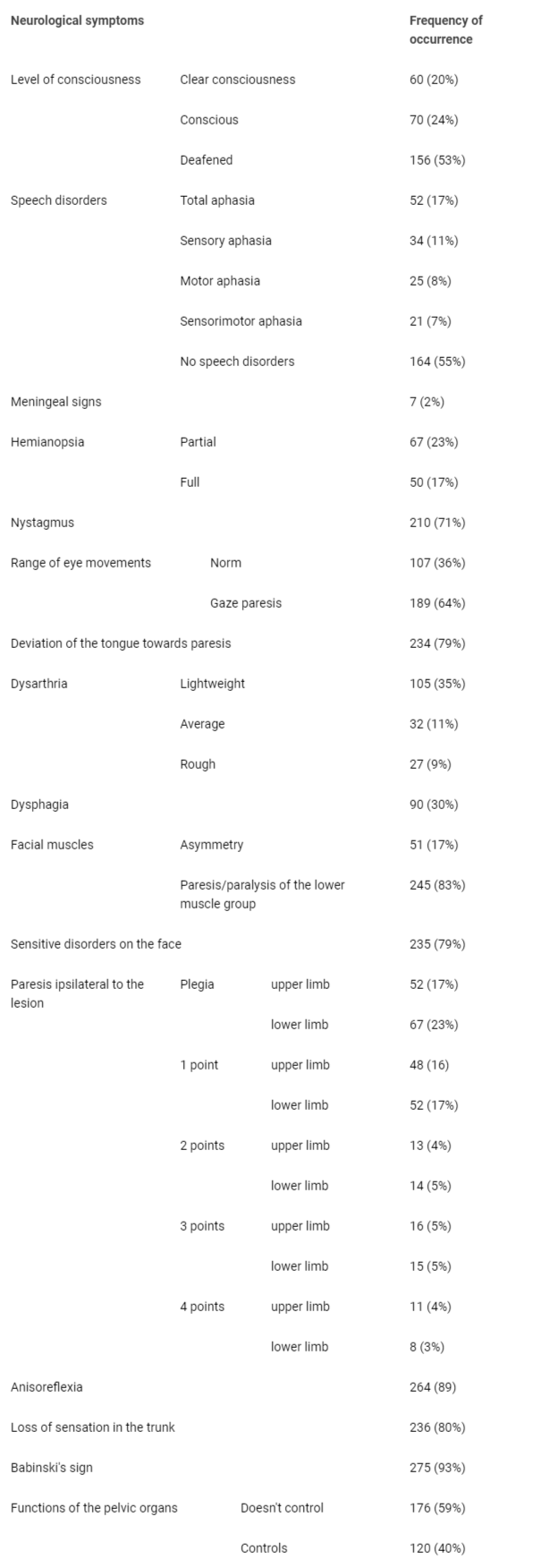
An analysis of the clinical picture of ischemic stroke was carried out in 296 patients with cerebrovascular accident in the carotid and vertebrobasilar areas (Table 1). When analyzing data from instrumental studies (CT, MRI) and the neurological status of patients, it was shown that in the territory of the left middle cerebral artery - 120 (40%), in the territory of the right middle cerebral artery - 141 (48%), in the territory of the right internal carotid artery - 17 (5.7%), in the basin of the left internal carotid artery -12 (4%), in the vertebrobasilar system -16 (5%). The underlying diseases were: arterial hypertension stage 3, degree 3 - 279 (94%), and atherosclerosis of the brachiocephalic arteries - 180 (61%). Concomitant diseases were: cardiac ischemia: atherosclerotic cardiosclerosis - 23.7%, post-infarction cardiosclerosis - 7.8%, chronic obstructive pulmonary diseases - 9.7%, varicose veins of the lower extremities - 22.7%, occlusive thrombosis of the subcutaneous and deep veins - 9 % (Table 2).
Table 2: Clinical characteristics of patients with IS non-cardioembolic pathogenetic variant according to TOAST criteria.
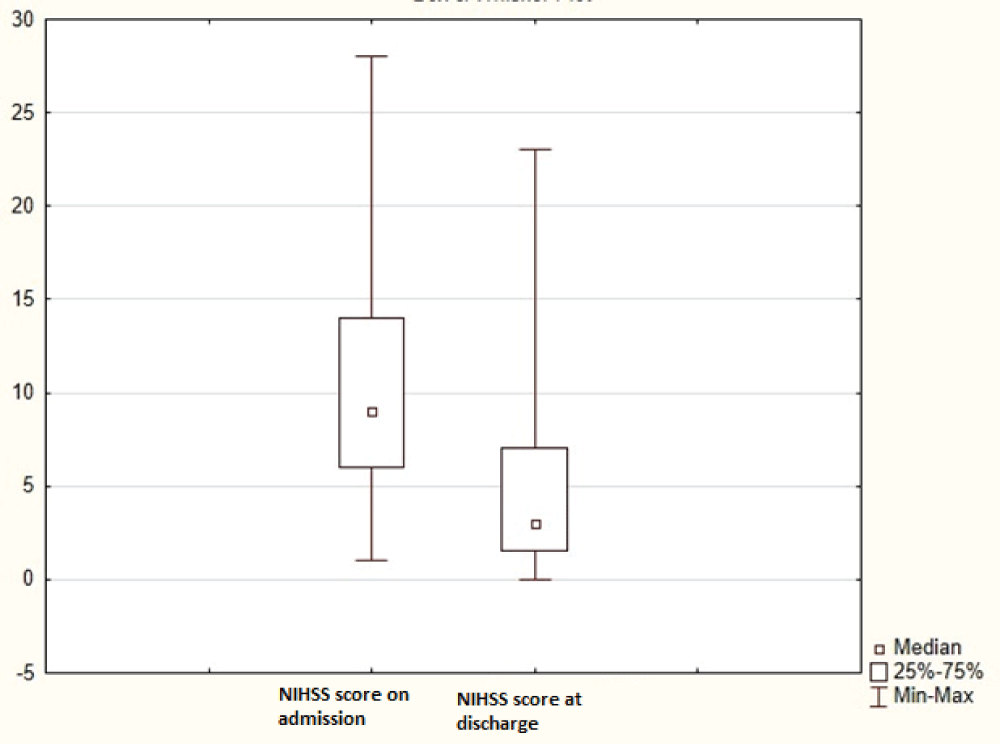
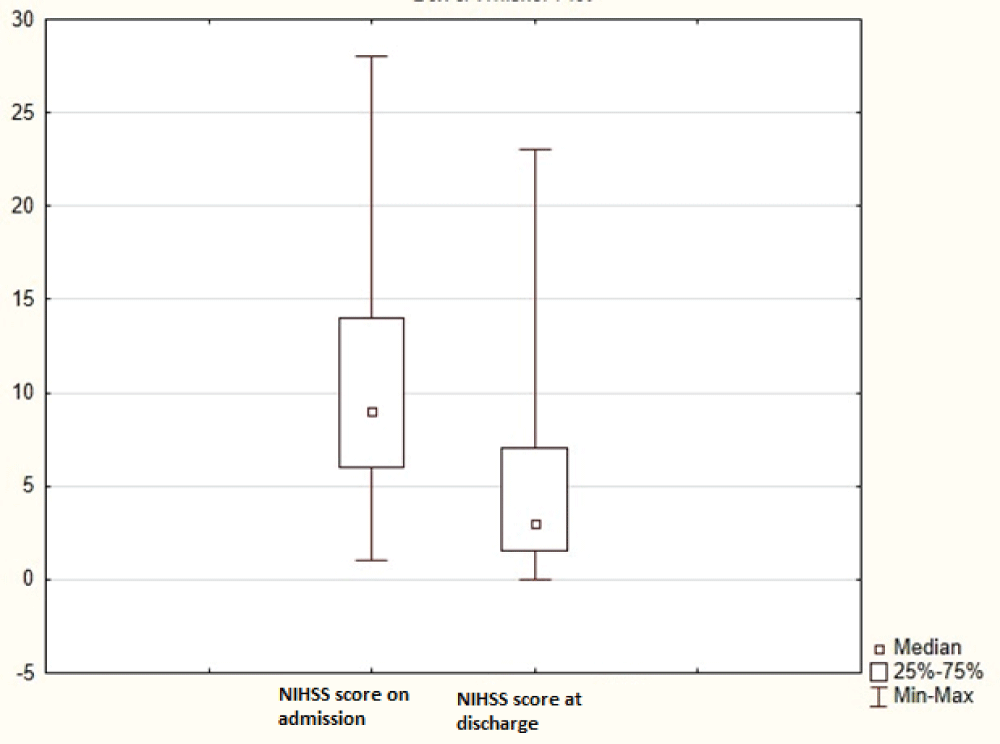
All patients showed positive dynamics at the time of discharge - NIHSS scores at discharge (9 [6;146;14Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993 Jan;24(1):35-41. doi: 10.1161/01.str.24.1.35. PMID: 7678184.]) were significantly lower than NIHSS scores at admission (3 [2;72;7Anisimova AV, Gunchenko AS, Avdonina MA, Ikonnikova AU, Nasedkina TV. Clinical features and genetic risk factors in the development of ischemic stroke. Ural Medical Journal. 2017; T. 153: 9.]) (p <0.0005) (Figure 1).
Figure 1: NIHSS scores at admission and discharge.
Blood was collected for genetic studies in tubes with EDTA. For DNA genetic analysis, the QIamp DNA Mini kit (Qiagen, Germany) and LumiPure genomic DNA Blood and Buccal Kit (Lumiprobe RUS Ltd., Russia) were used.
The aggregation properties of platelets in the presence of inducers (arachidonic acid, ristomycin, ADP, spontaneous aggregation) were studied on the 3rd day of taking aspirin at a dose of 125 mg using light transmission aggregometry.
The criterion for resistance to acetylsalicylic acid was a platelet aggregation level of ≥ 20% after induction with arachidonic acid and > 70% after induction with ADP. According to the study results, laboratory aspirin resistance was detected in 127 patients (43%), and aspirin sensitivity was detected in 169 (57%).
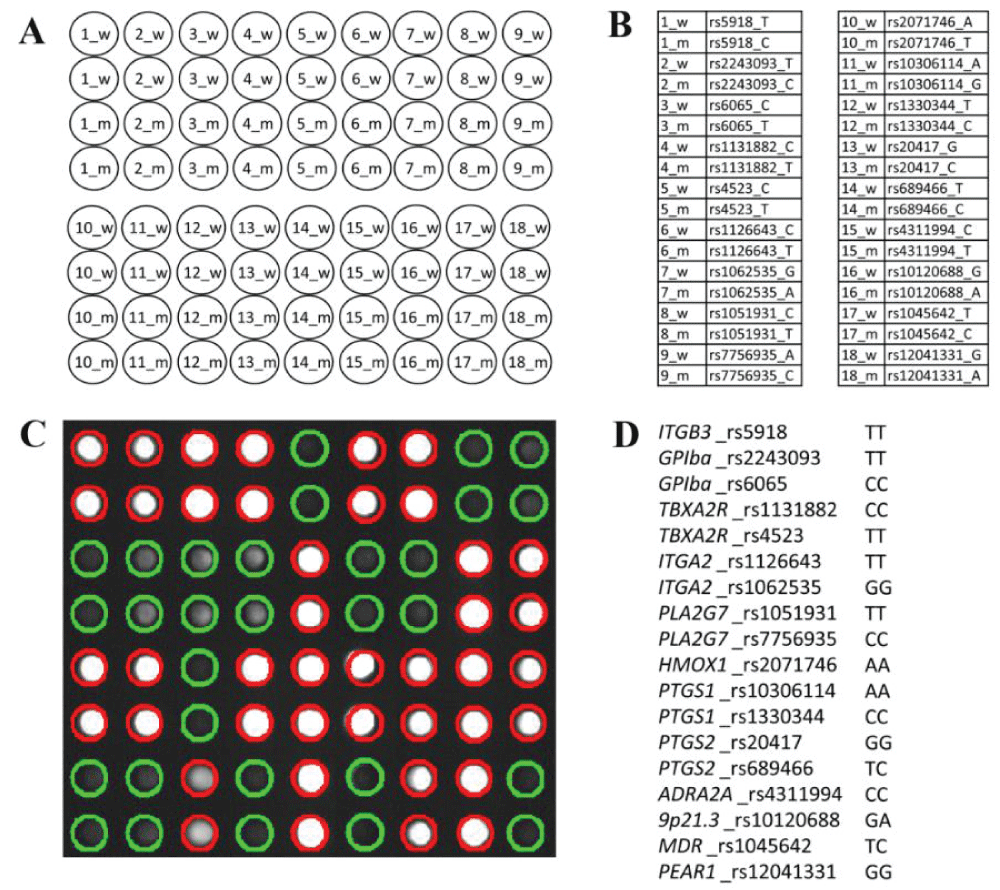
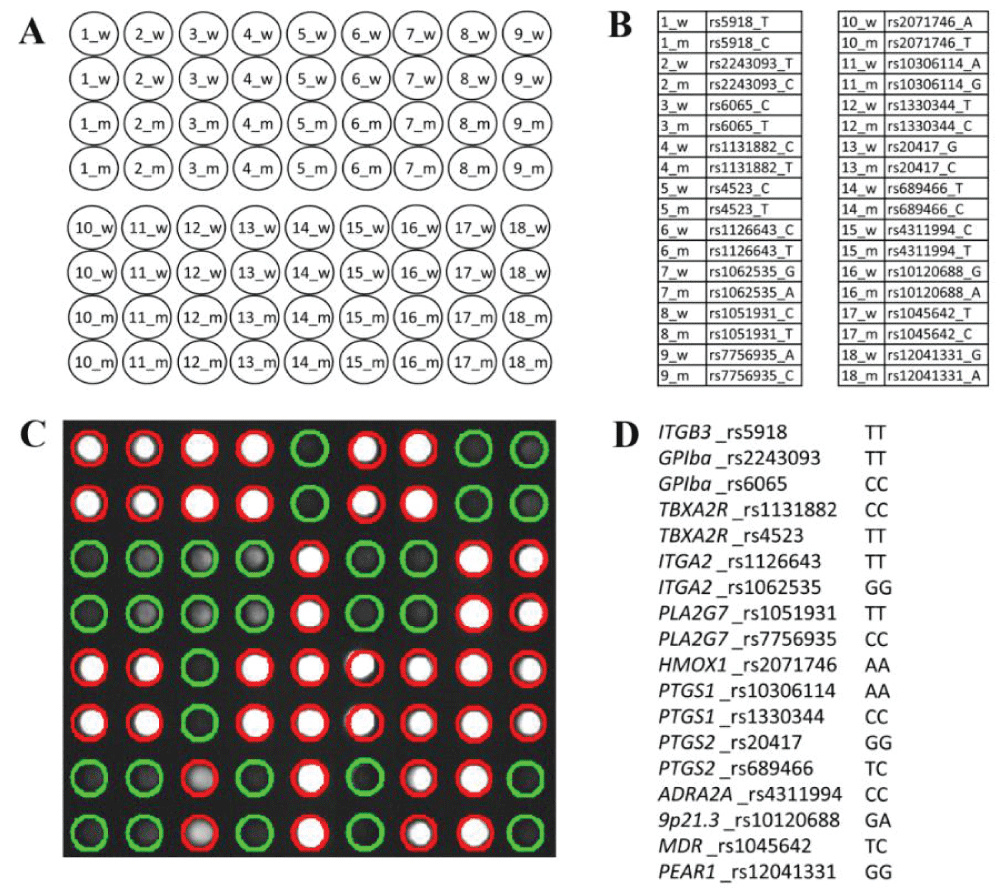
Based on the results of studying the literature data, genes were selected that are associated with changes in platelet aggregation properties. (eighteen SNPs in the ITGB3, GPIba, TBXA2R, ITGA2, PLA2G7, HMOX1, PTGS1, PTGS2, ADRA2A, ABCB1, PEAR1 genes and the 9p21.3 intergenic region) that were identified using low-density hydrogel biochip technology.
Statistical processing of the study data was carried out using Statistica 10 and Microsoft Excel. p values are before adjustment for multiple comparisons; after Bonferroni correction, all p values > 0.05.
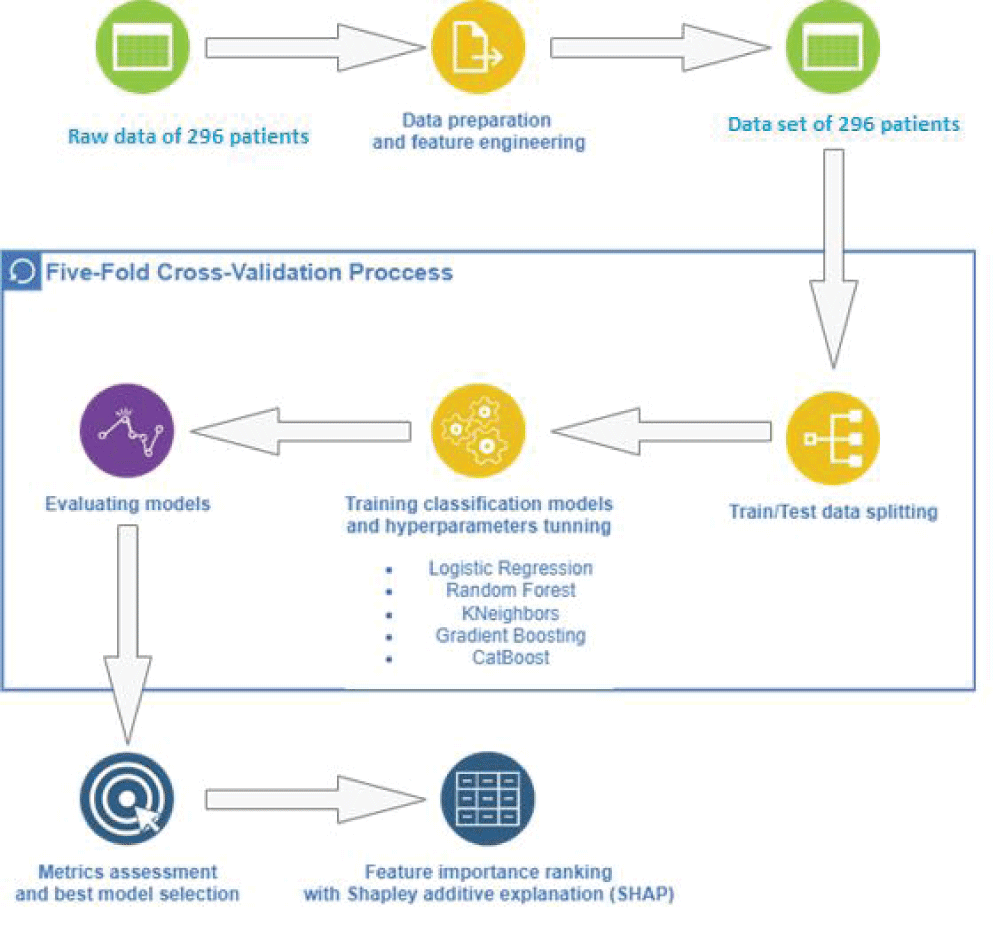
To understand the role of genetic markers and clinical and laboratory parameters in predicting noncardioembolic ischemic stroke, we developed Machine Learning (ML) systems. Specifically, we used the following classification algorithms implemented using Python: including Logistic Regression, Random Forest, KNeighbors, Gradient Boosting, and CatBoost [2525Dorogush Veronika A, Ershov V, Gulin A. CatBoost: Gradient boosting with categorical features support. ArXiv. 2018; arXiv: 1810.11363.,2626Lundberg Scott M, Lee S. A unified approach to interpreting model predictions. Adv. Neural Inf. Process. Syst. 2017; 30: 4768-4777.]. The flow of the ML procedure pipeline is shown in Figure 2.
Figure 2: Biological microchip for genetic marker analysis.
After a preliminary examination of the original data, we identified an imbalance in the class distribution, which necessitated a solution to the problem by increasing the minority class. Initial use of genetic attributes alone yielded limited predictive capabilities, which prompted us to refine the model to include both anthropometric and clinical details. The final set of features included age, Body Mass Index (BMI), TOAST type (Type), NHISS score on admission (NHISS), Ristocetin-induced platelet aggregation (Rist), Arachidonic Acid (AA) level, spontaneous platelet aggregation (Spontan)., High-Density Lipoprotein (HDL) and PTGS1 rs1330344 genes. Patient age was divided into groups and converted into a categorical feature.
All models were trained using five-fold Cross-Validation (CV). To ensure consistency, folds were stratified, keeping class proportions similar to the overall data set. The selection of optimal hyperparameters was carried out using the GridSearchCV library, which systematically explored a predefined parameter space to identify the most effective combinations. Particular attention was paid to optimizing the F1 score for all models.
Not surprisingly, CatBoost gradient boosting on decision trees outperformed other methods, which is attributed to its ability to exploit categorical feature information. The mean values of key performance indicators were: 0.8909 ± 0.0558 (AUC), 0.8181 ± 0.0579 (F1 score), 0.7876 ± 0.0883 (accuracy), and 0.8660 ± 0.0446 (recall).
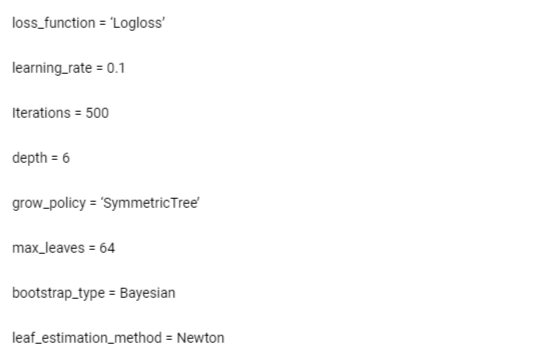
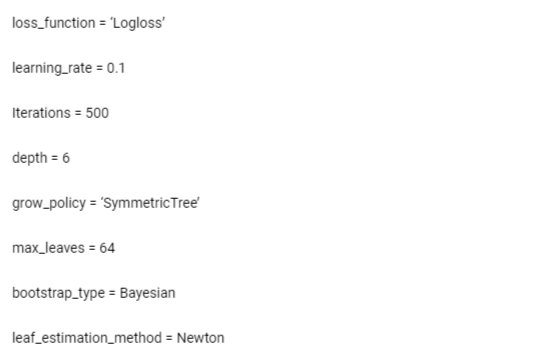
The optimal parameters that showed superior CV results can be found in Appendix A (Table 3).
Table 3 appendix a: Parameters of the Best-Performing Model
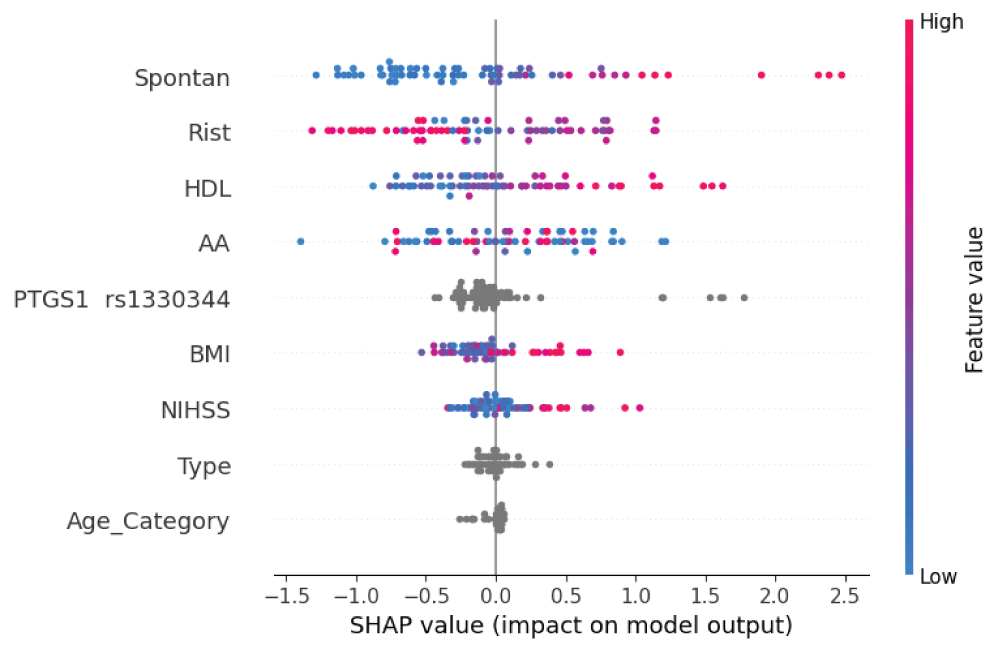
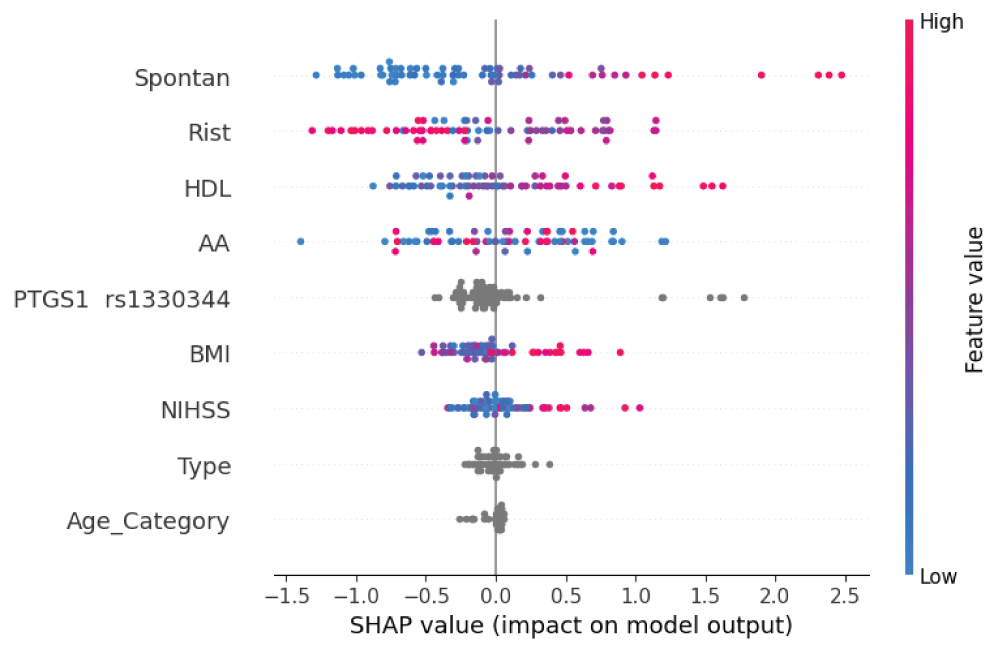
To assess the impact of individual features on model performance and highlight key factors, we conducted an additive analysis of Shapley’s explanations (Figure 2). This made it possible to understand the relationship of variables in the predicted scenario and their weight in the final assessment. Essentially, Shapley values shed light on the significance of a trait by relating the model’s predictions to the presence or absence of the trait. When considering the SHAPE plot (Figures 3,4), a positive effect on predicting recurrent stroke was observed for high levels of spontaneous platelet aggregation, admission NHISS score, and high-density lipoprotein cases. Conversely, there was a presumed attenuation of the prognosis for patients with low and average body mass index and an increase in the effect for high values. Points on the rs1330344 PTGS1 gene with high density on the negative side indicated the prevalence of predominant alleles, reducing the likelihood of predicting recurrent stroke using our model. However, their identification within the framework of Shapley’s analysis was considered impossible.
Figure 3: Machine learning pipeline.
Figure 4: Feature importance ranking obtained using SHAP values. Variables are listed in order of significance from top to bottom along the y-axis. Each dot represents a patient, and its color indicates the value of the corresponding variable. The position of the points on the x-axis represents SHAP values indicating changes in log odds, and the probability of success can be extracted from this value.
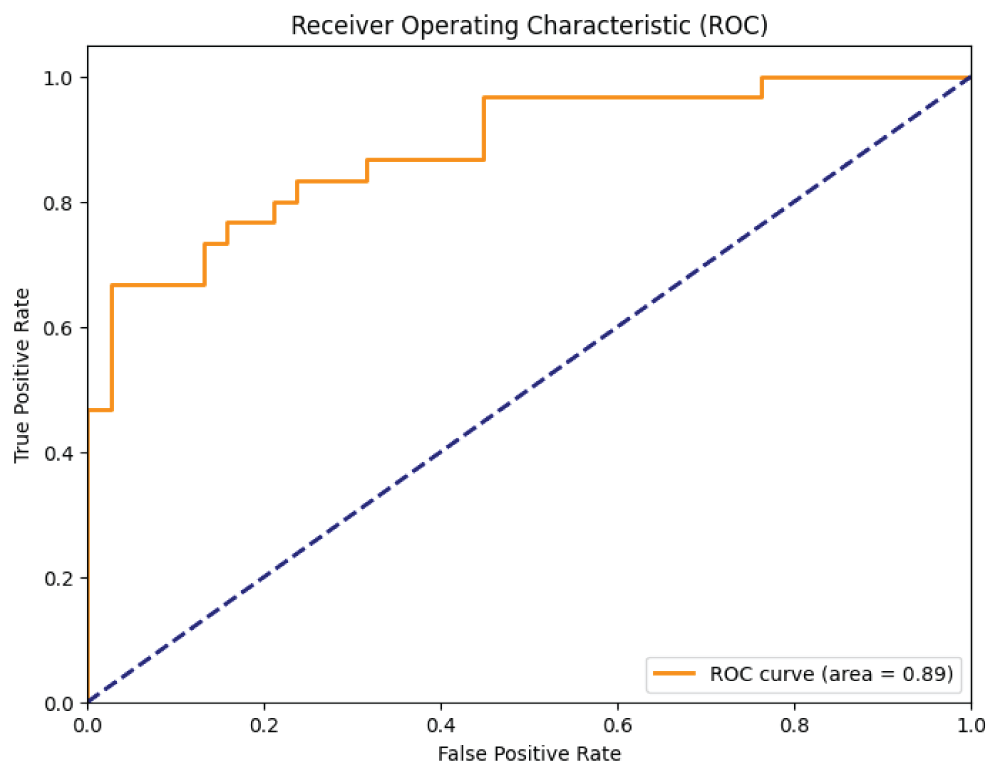
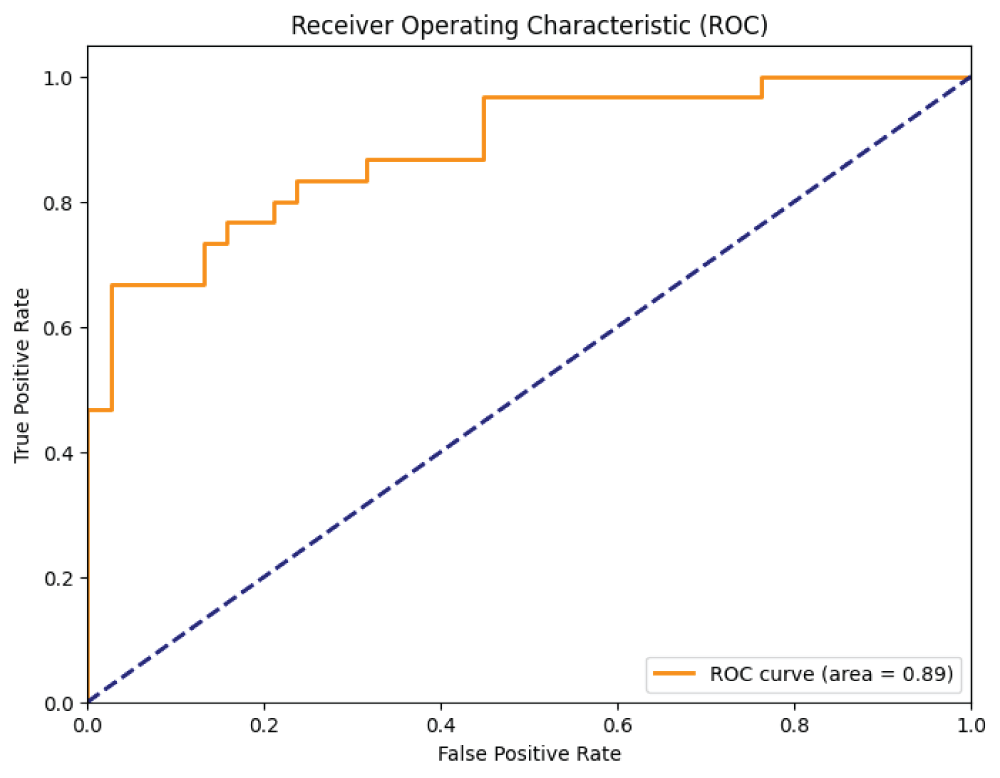
In our analysis, we used the Receiver Operating Characteristic (ROC) curve to evaluate the predictive performance of our model. This curve illustrates the trade-off between true positive rates (sensitivity) and false positive rates (1-specificity) at different thresholds. The Area Under the Curve (AUC) provides a single metric to evaluate the overall performance of the model. Our model demonstrated a commendable AUC of 0.8909 ± 0.0558, indicating excellent predictive capabilities. The optimal cut-off point, determined by maximizing the Youden index (sensitivity + specificity - 1), was determined to be 0.81. At this threshold, sensitivity was 67% and specificity was 97%.
The ROC curve not only visually depicts the balance between sensitivity and specificity, but also highlights the model’s ability to distinguish between positive and negative predictions. Its position above the no-discrimination line highlights the robustness of our model in making accurate discriminations.
DNA samples from 296 patients who suffered an ischemic stroke were genotyped. According to the study results, laboratory aspirin resistance was detected in 127 patients (43%), and aspirin sensitivity was detected in 169 (57%). Next, associations of gene polymorphisms with clinical and laboratory parameters were studied. For the first time, a model based on machine learning was developed and applied in a group of patients with laboratory aspirin resistance to assess the risks of recurrent ischemic strokes, taking into account clinical and genetic associations.
The CC genotype of the rs1330344 gene in the PTGS1 gene was more common in the AR group than in the AC group (9.4% vs. 4.1%; OR = 2.48, 95% CI = 0.93-6.60, p = 0.062), the difference is not statistically significant. In CC homozygotes of the PTGS1 rs1330344 genotype, the average rate of AK-induced aggregation was 55.4% higher than in the TT+CT genotypes (37.07 versus 23.86, p = 0.026). The mean ADP-induced aggregation was 14.8% higher in TT+CT rs4523 TBXA2R genotypes compared to CC genotypes (43.4 vs. 37.7; p = 0.031). The mean ADP-induced aggregation was 11.6% lower in AA+GA ITGA2 rs1062535 genotypes compared to GG homozygotes (39.25 vs. 44.17, p = 0.051). In GG homozygotes for rs1062535 in the ITGA2 gene, the dynamics of NIHSS indicators upon admission and at the time of discharge were significantly higher compared to the indicators of groups of patients with GA+AA genotypes (6.57 versus 5.3, p = 0.0008). We have identified polymorphic gene markers that are associated with the characteristics of the clinical course of the cerebrovascular process (against the background of a progressive critical course of arterial hypertension) and with pathogenetic variants of ischemic stroke (non-cardioembolic ischemic stroke), and the presence of other unmodified risk factors.
Thus, as a result of the study, associations of polymorphism of genes of the hemostatic system with parameters of platelet hemostasis, the dynamics of the clinical picture (scores on the NIHSS scale) in patients with ischemic stroke, as well as anthropometric data of patients were identified. have been identified. The study made it possible to identify an integral indicator that may be an unfavorable sign of recurrent ischemic stroke, which requires the development of an individual approach to the treatment process. The model used in this study made it possible to calculate the values of signs, both clinical and laboratory, that make a significant contribution to the prognosis of recurrent ischemic strokes in patients with aspirin resistance. Our model demonstrated an AUC of 0.8909 ± 0.0558, indicating excellent prediction ability. In our analysis, the Receiver Operating Characteristic (ROC) curve was used to evaluate the predictive ability of our model. The ROC curve plots the true positive rate (sensitivity) versus the false positive rate (specificity 1) for various cutoff values. The area under the curve (AUC) is the only measure of model performance: an AUC of 1.0 indicates perfect predictive ability, and an AUC of 0.5 suggests no predictive ability beyond chance (Figure 5). The optimal cut-off point, determined by maximizing the Youden index (sensitivity + specificity - 1), was 0.81. At this threshold, sensitivity was 67% and specificity was 97%. These features are likely to influence both a positive and a negative prognosis. The studied clinical and genetic features in the group of patients with laboratory aspirin resistance can be used to identify groups of patients at high risk of recurrent ischemic strokes and to develop personalized approaches to the prevention of recurrent ischemic strokes - the selection of individual antiplatelet therapy.
Anisimova AV, Gunchenko AS, Ikonnikova AY, Galkin SS, Avdonina MA, Nasedkina TV. Kliniko-geneticheskiĭ analiz faktorov riska razvitiia ostroĭ i khronicheskoĭ ishemii golovnogo mozga [A clinical and genetic analysis of risk factors for the development of acute and chronic cerebral ischemia]. Zh Nevrol Psikhiatr Im S S Korsakova. 2019;119(3. Vyp. 2):62-67. Russian. doi: 10.17116/jnevro201911903262. PMID: 31184626.
Anisimova AV, Gunchenko AS, Avdonina MA, Ikonnikova AU, Nasedkina TV. Clinical features and genetic risk factors in the development of ischemic stroke. Ural Medical Journal. 2017; T. 153: 9.
Anisimova AV, Gendlin GE, Borisov SN. [Prevention of stroke in patients with atrial fibrillation: a role of modern anticoagulants]. Zh Nevrol Psikhiatr Im S S Korsakova. 2013;113(9 Pt 2):62-9. Russian. PMID: 24107898.
Galkin SS, Gunchenko AS, Abdukhalikova Z, Yutskova EV, Anisimova AV. Dinamika pokazatelei trombotsitarnogo gemostaza u patsientov s kardioembolicheskim insul'tom [Dynamics of platelet hemostasis indices in patients with cardioembolic stroke against the background of atrial fibrillation]. Zh Nevrol Psikhiatr Im S S Korsakova. 2021;121(12. Vyp. 2):62-68. Russian. doi: 10.17116/jnevro202112112262. PMID: 35044128.
Storozhakov GI, Gendlin GE, Anisimova AV, Melekhov AV, Ostrovskaya YI. Taktika antigipertenzivnoĭ terapii u patsientov s gipertonicheskim krizom, oslozhnennym gemorragicheskim insul'tom [Tactics of antihypertensive therapy in patients with hypertonic crisis complicated with hemorrhagic stroke]. Zh Nevrol Psikhiatr Im S S Korsakova. 2015;115(3 Pt 2):12-19. Russian. doi: 10.17116/jnevro2015115312-19. PMID: 26120992.
Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993 Jan;24(1):35-41. doi: 10.1161/01.str.24.1.35. PMID: 7678184.
Saini V, Guada L, Yavagal DR. Global Epidemiology of Stroke and Access to Acute Ischemic Stroke Interventions. Neurology. 2021 Nov 16;97(20 Suppl 2):S6-S16. doi: 10.1212/WNL.0000000000012781. PMID: 34785599.
Potter TBH, Tannous J, Vahidy FS. A Contemporary Review of Epidemiology, Risk Factors, Etiology, and Outcomes of Premature Stroke. Curr Atheroscler Rep. 2022 Dec;24(12):939-948. doi: 10.1007/s11883-022-01067-x. Epub 2022 Nov 14. PMID: 36374365; PMCID: PMC9660017.
Feigin VL, Brainin M, Norrving B, Martins S, Sacco RL, Hacke W, Fisher M, Pandian J, Lindsay P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int J Stroke. 2022 Jan;17(1):18-29. doi: 10.1177/17474930211065917. Erratum in: Int J Stroke. 2022 Apr;17(4):478. PMID: 34986727.
Pohl M, Hesszenberger D, Kapus K, Meszaros J, Feher A, Varadi I, Pusch G, Fejes E, Tibold A, Feher G. Ischemic stroke mimics: A comprehensive review. J Clin Neurosci. 2021 Nov;93:174-182. doi: 10.1016/j.jocn.2021.09.025. Epub 2021 Sep 20. PMID: 34656244.
Zheng S, Yao B. Impact of risk factors for recurrence after the first ischemic stroke in adults: A systematic review and meta-analysis. J Clin Neurosci. 2019 Feb;60:24-30. doi: 10.1016/j.jocn.2018.10.026. Epub 2018 Oct 16. PMID: 30340974.
Fernández-Cadenas I, Mendióroz M, Giralt D, Nafria C, Garcia E, Carrera C, Gallego-Fabrega C, Domingues-Montanari S, Delgado P, Ribó M, Castellanos M, Martínez S, Freijo M, Jiménez-Conde J, Rubiera M, Alvarez-Sabín J, Molina CA, Font MA, Grau Olivares M, Palomeras E, Perez de la Ossa N, Martinez-Zabaleta M, Masjuan J, Moniche F, Canovas D, Piñana C, Purroy F, Cocho D, Navas I, Tejero C, Aymerich N, Cullell N, Muiño E, Serena J, Rubio F, Davalos A, Roquer J, Arenillas JF, Martí-Fábregas J, Keene K, Chen WM, Worrall B, Sale M, Arboix A, Krupinski J, Montaner J; GRECOS Study Group. GRECOS Project (Genotyping Recurrence Risk of Stroke): The Use of Genetics to Predict the Vascular Recurrence After Stroke. Stroke. 2017 May;48(5):1147-1153. doi: 10.1161/STROKEAHA.116.014322. Epub 2017 Apr 14. PMID: 28411264; PMCID: PMC5473776.
Pezzini A, Grassi M, Del Zotto E, Lodigiani C, Ferrazzi P, Spalloni A, Patella R, Giossi A, Volonghi I, Iacoviello L, Magoni M, Rota LL, Rasura M, Padovani A. Common genetic markers and prediction of recurrent events after ischemic stroke in young adults. Neurology. 2009 Sep 1;73(9):717-23. doi: 10.1212/WNL.0b013e3181b59aaf. PMID: 19720979.
Ding L, Liu Y, Meng X, Jiang Y, Lin J, Cheng S, Xu Z, Zhao X, Li H, Wang Y, Li Z. Biomarker and genomic analyses reveal molecular signatures of non-cardioembolic ischemic stroke. Signal Transduct Target Ther. 2023 May 30;8(1):222. doi: 10.1038/s41392-023-01465-w. PMID: 37248226; PMCID: PMC10227023.
Dash P, Singh VK, Gautam D, Pathak A, Kumar A, Mishra SP, Dash D, Mishra VN, Joshi D, Chaurasia RN. Aspirin resistance and blood biomarkers in predicting ischemic stroke recurrence: An exploratory study. Brain Circ. 2022 Mar 21;8(1):31-37. doi: 10.4103/bc.bc_75_21. PMID: 35372727; PMCID: PMC8973447.
Parsa-Kondelaji M, Mansouritorghabeh H. Aspirin and clopidogrel resistance; a neglected gap in stroke and cardiovascular practice in Iran: a systematic review and meta-analysis. Thromb J. 2023 Jul 27;21(1):79. doi: 10.1186/s12959-023-00522-2. PMID: 37501091; PMCID: PMC10373335.
Ross S, Krebs K, Paré G, Milani L. Pharmacogenomics in Stroke and Cardiovascular Disease: State of the Art. Stroke. 2023 Jan;54(1):270-278. doi: 10.1161/STROKEAHA.122.037717. Epub 2022 Nov 3. PMID: 36325912.
Morton M, Kubiak-Balcerewicz K, Sarnowska A, Fiszer U. Biochemical aspirin resistance in acute stroke patients and its association with clinical factors: a prospective pilot study. Folia Neuropathol. 2021;59(3):271-275. doi: 10.5114/fn.2021.109434. PMID: 34628792.
Wang H, Yuan J, Wang Y, Chen J. To study the mechanism of panax notoginseng in the treatment of aspirin resistance in the secondary prevention of stroke based on TLR4/MyD88/NF-κB signaling pathway: A study protocol. Medicine (Baltimore). 2022 Dec 16;101(50):e31919. doi: 10.1097/MD.0000000000031919. PMID: 36550905; PMCID: PMC9771212.
Venketasubramanian N, Agustin SJ, Padilla JL, Yumul MP, Sum C, Lee SH, Ponnudurai K, Gan RN. Comparison of Different Laboratory Tests to Identify "Aspirin Resistance" and Risk of Vascular Events among Ischaemic Stroke Patients: A Double-Blind Study. J Cardiovasc Dev Dis. 2022 May 12;9(5):156. doi: 10.3390/jcdd9050156. PMID: 35621867; PMCID: PMC9145610.
Li Z, Dong W, Yang D, Sun L, He X, Hu H, Zhang J, Wang C, Li Y, Zhao M, Kong Y, Wang Y. Body weight, CYP2C19, and P2Y12 receptor polymorphisms relate to clopidogrel resistance in a cohort of Chinese ischemic stroke patients with aspirin intolerance. Eur J Clin Pharmacol. 2020 Nov;76(11):1517-1527. doi: 10.1007/s00228-020-02946-5. Epub 2020 Jul 6. PMID: 32632713.
Wiśniewski A, Filipska K, Sikora J, Kozera G. Aspirin Resistance Affects Medium-Term Recurrent Vascular Events after Cerebrovascular Incidents: A Three-Year Follow-up Study. Brain Sci. 2020 Mar 19;10(3):179. doi: 10.3390/brainsci10030179. PMID: 32204465; PMCID: PMC7139350.
Alhazzani A, Venkatachalapathy P, Padhilahouse S, Sellappan M, Munisamy M, Sekaran M, Kumar A. Biomarkers for Antiplatelet Therapies in Acute Ischemic Stroke: A Clinical Review. Front Neurol. 2021 Jun 10;12:667234. doi: 10.3389/fneur.2021.667234. PMID: 34177775; PMCID: PMC8222621.
Silva GFD, Lopes BM, Moser V, Ferreira LE. Impact of pharmacogenetics on aspirin resistance: a systematic review. Arq Neuropsiquiatr. 2023 Jan;81(1):62-73. doi: 10.1055/s-0042-1758445. Epub 2023 Mar 14. PMID: 36918009; PMCID: PMC10014202.
Dorogush Veronika A, Ershov V, Gulin A. CatBoost: Gradient boosting with categorical features support. ArXiv. 2018; arXiv: 1810.11363.
Lundberg Scott M, Lee S. A unified approach to interpreting model predictions. Adv. Neural Inf. Process. Syst. 2017; 30: 4768-4777.
Anisimova AN, Galkin SE, Gunchenko AN, Nasedkina TA, Vorobiev IG. The Model for Clinical, Laboratory, and Genetic Prediction of Recurrent Ischemic Stroke against the Background of Laboratory Aspirin Resistance using Machine Learning. IgMin Res. 30 Jan, 2024; 2(1): 034-044. IgMin ID: igmin143; DOI: 10.61927/igmin143; Available at: www.igminresearch.com/articles/pdf/igmin143.pdf
1Pirogov Russian National Research Medical University, Ministry of Health of the Russian Federation, Moscow, Russia
2Engelhardt Institute of Molecular Biology RAS, Moscow, Russia
Address Correspondence: Sergey S Galkin, Pirogov Russian National Research Medical University, Ministry of Health of the Russian Federation, Moscow, Russia, Email: [email protected]
How to cite this article: Anisimova AN, Galkin SE, Gunchenko AN, Nasedkina TA, Vorobiev IG. The Model for Clinical, Laboratory, and Genetic Prediction of Recurrent Ischemic Stroke against the Background of Laboratory Aspirin Resistance using Machine Learning. IgMin Res. 30 Jan, 2024; 2(1): 034-044. IgMin ID: igmin143; DOI: 10.61927/igmin143; Available at: www.igminresearch.com/articles/pdf/igmin143.pdf
Table 1: Median values of the main clinical and laboratory ...
Table 2: Clinical characteristics of patients with IS non-c...
Table 3: Appendix A: Parameters of the Best-Performing Model...
Anisimova AV, Gunchenko AS, Ikonnikova AY, Galkin SS, Avdonina MA, Nasedkina TV. Kliniko-geneticheskiĭ analiz faktorov riska razvitiia ostroĭ i khronicheskoĭ ishemii golovnogo mozga [A clinical and genetic analysis of risk factors for the development of acute and chronic cerebral ischemia]. Zh Nevrol Psikhiatr Im S S Korsakova. 2019;119(3. Vyp. 2):62-67. Russian. doi: 10.17116/jnevro201911903262. PMID: 31184626.
Anisimova AV, Gunchenko AS, Avdonina MA, Ikonnikova AU, Nasedkina TV. Clinical features and genetic risk factors in the development of ischemic stroke. Ural Medical Journal. 2017; T. 153: 9.
Anisimova AV, Gendlin GE, Borisov SN. [Prevention of stroke in patients with atrial fibrillation: a role of modern anticoagulants]. Zh Nevrol Psikhiatr Im S S Korsakova. 2013;113(9 Pt 2):62-9. Russian. PMID: 24107898.
Galkin SS, Gunchenko AS, Abdukhalikova Z, Yutskova EV, Anisimova AV. Dinamika pokazatelei trombotsitarnogo gemostaza u patsientov s kardioembolicheskim insul'tom [Dynamics of platelet hemostasis indices in patients with cardioembolic stroke against the background of atrial fibrillation]. Zh Nevrol Psikhiatr Im S S Korsakova. 2021;121(12. Vyp. 2):62-68. Russian. doi: 10.17116/jnevro202112112262. PMID: 35044128.
Storozhakov GI, Gendlin GE, Anisimova AV, Melekhov AV, Ostrovskaya YI. Taktika antigipertenzivnoĭ terapii u patsientov s gipertonicheskim krizom, oslozhnennym gemorragicheskim insul'tom [Tactics of antihypertensive therapy in patients with hypertonic crisis complicated with hemorrhagic stroke]. Zh Nevrol Psikhiatr Im S S Korsakova. 2015;115(3 Pt 2):12-19. Russian. doi: 10.17116/jnevro2015115312-19. PMID: 26120992.
Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993 Jan;24(1):35-41. doi: 10.1161/01.str.24.1.35. PMID: 7678184.
Saini V, Guada L, Yavagal DR. Global Epidemiology of Stroke and Access to Acute Ischemic Stroke Interventions. Neurology. 2021 Nov 16;97(20 Suppl 2):S6-S16. doi: 10.1212/WNL.0000000000012781. PMID: 34785599.
Potter TBH, Tannous J, Vahidy FS. A Contemporary Review of Epidemiology, Risk Factors, Etiology, and Outcomes of Premature Stroke. Curr Atheroscler Rep. 2022 Dec;24(12):939-948. doi: 10.1007/s11883-022-01067-x. Epub 2022 Nov 14. PMID: 36374365; PMCID: PMC9660017.
Feigin VL, Brainin M, Norrving B, Martins S, Sacco RL, Hacke W, Fisher M, Pandian J, Lindsay P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int J Stroke. 2022 Jan;17(1):18-29. doi: 10.1177/17474930211065917. Erratum in: Int J Stroke. 2022 Apr;17(4):478. PMID: 34986727.
Pohl M, Hesszenberger D, Kapus K, Meszaros J, Feher A, Varadi I, Pusch G, Fejes E, Tibold A, Feher G. Ischemic stroke mimics: A comprehensive review. J Clin Neurosci. 2021 Nov;93:174-182. doi: 10.1016/j.jocn.2021.09.025. Epub 2021 Sep 20. PMID: 34656244.
Zheng S, Yao B. Impact of risk factors for recurrence after the first ischemic stroke in adults: A systematic review and meta-analysis. J Clin Neurosci. 2019 Feb;60:24-30. doi: 10.1016/j.jocn.2018.10.026. Epub 2018 Oct 16. PMID: 30340974.
Fernández-Cadenas I, Mendióroz M, Giralt D, Nafria C, Garcia E, Carrera C, Gallego-Fabrega C, Domingues-Montanari S, Delgado P, Ribó M, Castellanos M, Martínez S, Freijo M, Jiménez-Conde J, Rubiera M, Alvarez-Sabín J, Molina CA, Font MA, Grau Olivares M, Palomeras E, Perez de la Ossa N, Martinez-Zabaleta M, Masjuan J, Moniche F, Canovas D, Piñana C, Purroy F, Cocho D, Navas I, Tejero C, Aymerich N, Cullell N, Muiño E, Serena J, Rubio F, Davalos A, Roquer J, Arenillas JF, Martí-Fábregas J, Keene K, Chen WM, Worrall B, Sale M, Arboix A, Krupinski J, Montaner J; GRECOS Study Group. GRECOS Project (Genotyping Recurrence Risk of Stroke): The Use of Genetics to Predict the Vascular Recurrence After Stroke. Stroke. 2017 May;48(5):1147-1153. doi: 10.1161/STROKEAHA.116.014322. Epub 2017 Apr 14. PMID: 28411264; PMCID: PMC5473776.
Pezzini A, Grassi M, Del Zotto E, Lodigiani C, Ferrazzi P, Spalloni A, Patella R, Giossi A, Volonghi I, Iacoviello L, Magoni M, Rota LL, Rasura M, Padovani A. Common genetic markers and prediction of recurrent events after ischemic stroke in young adults. Neurology. 2009 Sep 1;73(9):717-23. doi: 10.1212/WNL.0b013e3181b59aaf. PMID: 19720979.
Ding L, Liu Y, Meng X, Jiang Y, Lin J, Cheng S, Xu Z, Zhao X, Li H, Wang Y, Li Z. Biomarker and genomic analyses reveal molecular signatures of non-cardioembolic ischemic stroke. Signal Transduct Target Ther. 2023 May 30;8(1):222. doi: 10.1038/s41392-023-01465-w. PMID: 37248226; PMCID: PMC10227023.
Dash P, Singh VK, Gautam D, Pathak A, Kumar A, Mishra SP, Dash D, Mishra VN, Joshi D, Chaurasia RN. Aspirin resistance and blood biomarkers in predicting ischemic stroke recurrence: An exploratory study. Brain Circ. 2022 Mar 21;8(1):31-37. doi: 10.4103/bc.bc_75_21. PMID: 35372727; PMCID: PMC8973447.
Parsa-Kondelaji M, Mansouritorghabeh H. Aspirin and clopidogrel resistance; a neglected gap in stroke and cardiovascular practice in Iran: a systematic review and meta-analysis. Thromb J. 2023 Jul 27;21(1):79. doi: 10.1186/s12959-023-00522-2. PMID: 37501091; PMCID: PMC10373335.
Ross S, Krebs K, Paré G, Milani L. Pharmacogenomics in Stroke and Cardiovascular Disease: State of the Art. Stroke. 2023 Jan;54(1):270-278. doi: 10.1161/STROKEAHA.122.037717. Epub 2022 Nov 3. PMID: 36325912.
Morton M, Kubiak-Balcerewicz K, Sarnowska A, Fiszer U. Biochemical aspirin resistance in acute stroke patients and its association with clinical factors: a prospective pilot study. Folia Neuropathol. 2021;59(3):271-275. doi: 10.5114/fn.2021.109434. PMID: 34628792.
Wang H, Yuan J, Wang Y, Chen J. To study the mechanism of panax notoginseng in the treatment of aspirin resistance in the secondary prevention of stroke based on TLR4/MyD88/NF-κB signaling pathway: A study protocol. Medicine (Baltimore). 2022 Dec 16;101(50):e31919. doi: 10.1097/MD.0000000000031919. PMID: 36550905; PMCID: PMC9771212.
Venketasubramanian N, Agustin SJ, Padilla JL, Yumul MP, Sum C, Lee SH, Ponnudurai K, Gan RN. Comparison of Different Laboratory Tests to Identify "Aspirin Resistance" and Risk of Vascular Events among Ischaemic Stroke Patients: A Double-Blind Study. J Cardiovasc Dev Dis. 2022 May 12;9(5):156. doi: 10.3390/jcdd9050156. PMID: 35621867; PMCID: PMC9145610.
Li Z, Dong W, Yang D, Sun L, He X, Hu H, Zhang J, Wang C, Li Y, Zhao M, Kong Y, Wang Y. Body weight, CYP2C19, and P2Y12 receptor polymorphisms relate to clopidogrel resistance in a cohort of Chinese ischemic stroke patients with aspirin intolerance. Eur J Clin Pharmacol. 2020 Nov;76(11):1517-1527. doi: 10.1007/s00228-020-02946-5. Epub 2020 Jul 6. PMID: 32632713.
Wiśniewski A, Filipska K, Sikora J, Kozera G. Aspirin Resistance Affects Medium-Term Recurrent Vascular Events after Cerebrovascular Incidents: A Three-Year Follow-up Study. Brain Sci. 2020 Mar 19;10(3):179. doi: 10.3390/brainsci10030179. PMID: 32204465; PMCID: PMC7139350.
Alhazzani A, Venkatachalapathy P, Padhilahouse S, Sellappan M, Munisamy M, Sekaran M, Kumar A. Biomarkers for Antiplatelet Therapies in Acute Ischemic Stroke: A Clinical Review. Front Neurol. 2021 Jun 10;12:667234. doi: 10.3389/fneur.2021.667234. PMID: 34177775; PMCID: PMC8222621.
Silva GFD, Lopes BM, Moser V, Ferreira LE. Impact of pharmacogenetics on aspirin resistance: a systematic review. Arq Neuropsiquiatr. 2023 Jan;81(1):62-73. doi: 10.1055/s-0042-1758445. Epub 2023 Mar 14. PMID: 36918009; PMCID: PMC10014202.
Dorogush Veronika A, Ershov V, Gulin A. CatBoost: Gradient boosting with categorical features support. ArXiv. 2018; arXiv: 1810.11363.
Lundberg Scott M, Lee S. A unified approach to interpreting model predictions. Adv. Neural Inf. Process. Syst. 2017; 30: 4768-4777.
The Model for Clinical, Laboratory, and Genetic Prediction of Recurrent Ischemic Stroke against the Background of Laboratory Aspirin Resistance using Machine Learning



 スキャンしてリンクを取得
スキャンしてリンクを取得